Playlist
Show Playlist
Hide Playlist
Beta and Calcium Channel Blockers – Hypertension


-
Slides 07 Cardiology Alpert.pdf
-
Download Lecture Overview
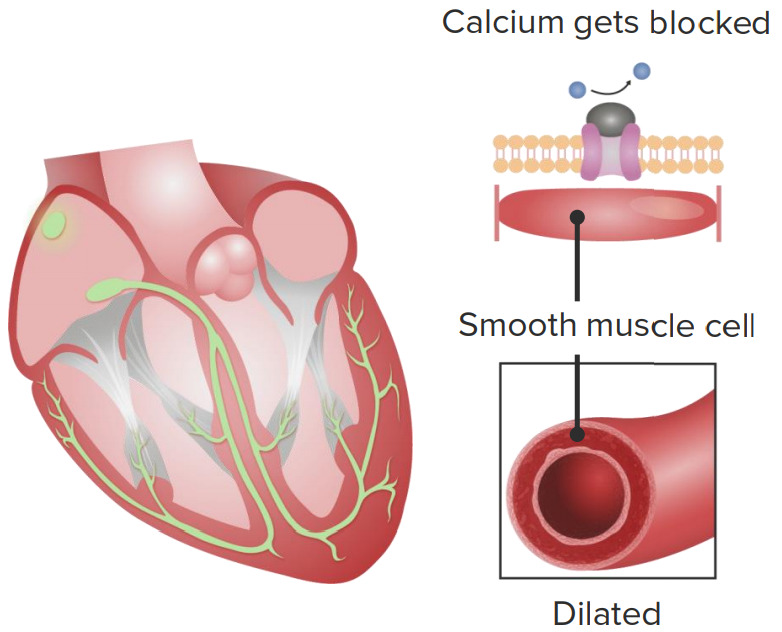
00:00 Well, let’s talk about Beta Blockers. We talked about these drugs both for heart failure and also for patients with ischemic heart disease, angina and heart attacks - myocardial infarction. Beta Blockers block the effect of adrenaline on the heart cells. What do they do by that? They slow the heart rate. They work on the sinus node and they work on other electrical components of the heart and they decrease the heart rate. By decreasing the heart rate, you decrease the work of the heart, you decrease the cardiac output, the amount of blood coming out. So, you also lower the blood pressure. So, Beta Blockers lower blood pressure and they lower the heart rate. They are not first line drugs because they're not quite as effective as the ACE inhibitors and the ARB’s and the thiazide diuretics. 00:46 So, sort of the front line troops in the control of hypertension are thiazide diuretics, ACE inhibitors, angiotensin receptor blockers. The second line of defense is Beta Blockers. 00:58 Now, on the other hand, if you have a patient who has ischemic heart disease and angina, then Beta Blockers move up to first place particularly if the patient has both hypertension and ischemic heart disease. You also want to lower the heart rate. So, you’re getting, if you will, two actions for the price of one when you use Beta Blockers in a patient with both high blood pressure and ischemic heart disease and those patients are extremely common. So, Beta Blockers are very, very commonly prescribed for these patients. 01:29 Here’s a list of a whole bunch of Beta Blockers. They're all generic, are just about all generic these days. The favorite one for heart failure tends to be carvedilol. The favorite one for blood pressure tends to be the metoprolol or atenolol, but again, all of them work and all of them are generic and inexpensive. You have to watch Beta Blockers for adverse effects. So, there’s a tendency by Beta Blockers to actually cause fluid retention and if that happens, if the patient has heart failure, you might at least initially make their heart failure a little worse. Down the road, the Beta Blockers actually help in heart failure, but initially when you first give them, you may have some fluid retention. 02:11 There are a number of other potential side effects. For example, if you’re an asthmatic, your asthma may get worse with Beta Blockers. Some… There are some central nervous systems effects… central nervous system effects. People may be a little depressed or tired who are on Beta Blockers. And so, of course, they can also excessively lower your heart rate or your blood pressure so you’re very fatigued or lightheaded and so forth. So, again, you start with a low dose and you advance carefully and watch for adversive effects or so called side effects. There’s another category of drugs called the calcium channel blockers. These drugs are potent vasodilators. They open up the small blood vessels in the periphery and they markedly reduce peripheral vascular resistance. 02:58 In fact, some people who get them, you can actually see their face becomes a little bit flushed because the small blood vessels are being opened up by this drug. There are two types of calcium channel blockers. There’s one that actually also can slow the heart rate down, those are the so called non-dihydroperidine calcium blockers - diltiazem and verapamil and they’re sometimes used for control of arrhythmias, for example, in atrial fibrillation to help control the heart rate. The non… The dihydroperidine calcium blockers, drugs like nifedipine, don’t have any electrical activity in the heart, but they dilate… both drugs dilate the periphery and lower the blood pressure. And so, often, particularly in patients with kidney disease, we’ll use a combination of an ACE inhibitor or an angiotensin receptor blocker and a dihydroperidine calcium blocker. That seems to be particularly effective and actually, may preserve kidney function in somebody who already has mild damage to the kidney. Both those drugs are commonly used to control high blood pressure in diabetics who, as you know, have a high risk of kidney injury.
About the Lecture
The lecture Beta and Calcium Channel Blockers – Hypertension by Joseph Alpert, MD is from the course Cardiac Diseases.
Included Quiz Questions
Beta blockers are considered first-line anti-hypertensive drugs in hypertensive patients with which of the following comorbidities?
- Ischemic heart disease
- Diabetes
- Sarcoidosis
- Irritable bowel syndrome
- Stroke
Which of the following anti-hypertensive medications is considered first-line therapy for patients with hypertension combined with abnormal kidney function?
- Amlodipine
- Furosemide
- Amiloride
- Spironolactone
- Atenolol
Author of lecture Beta and Calcium Channel Blockers – Hypertension

Joseph Alpert, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
