Playlist
Show Playlist
Hide Playlist
Asthma: Differential Diagnosis




-
Slides ObstructiveLungDisease Asthma RespiratoryPathology.pdf
-
Download Lecture Overview
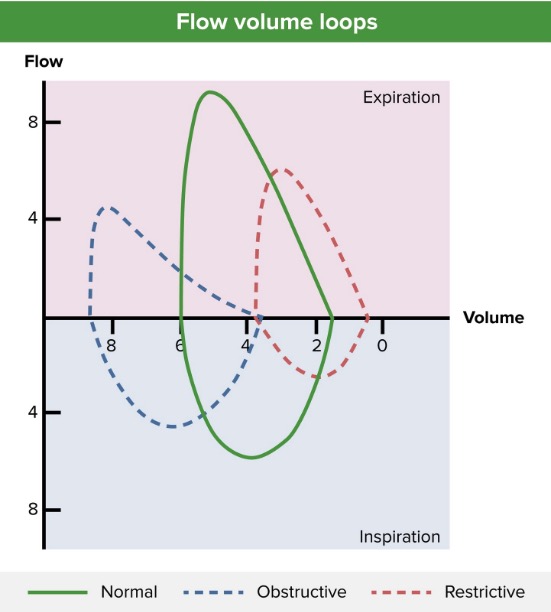
00:01 Now, multi-step approach to asthma. Remember, often times, with asthma, it is not, not present by itself. When it is present by other issues and you find other concomitant type of diseases well things become a little tricky. Often times your patient with asthma, well COPD, smoking history. What does a low DLCO mean to you? Remember diffusion capacity of your carbon monoxide is measuring how quickly is that oxygen leaving the alveoli entering? Good, the pulmonary capillaries. So therefore if there is increase mucous plug and there is increase barrier, then please understand that now, this type of COPD which is what asthma is right, it comes in umbrella of COPD. Well, now you have problems. Severe, chronic productive cough. Cor pulmonale, what does that mean? There is so much obstruction taking place that may result in pulmonary hypertension, therefore, resulting in right-sided heart failure. Is that cor pulmonale? Yes, it is. 01:06 Now, as we move on into further topics, I’ll give you the exact definition of COPD, asthma and its symptoms early on, really would not fit the definition and criteria of COPD so when we get to that point I’ll show you how chronic bronchitis, emphysema and asthma are all going to overlap. Take a look at low DLCO, smoking history. All of these is suggesting pretty severe disease. There could be vocal cord dysfunction. 01:35 Now, something that we talked about earlier which is your loop spirometry is that if there was vocal cord type of lesion which is, well, as you’re trying to breathe out say that there is especially any health care workers, then you have fixed type of obstruction. What does fixed obstruction mean to you? It means that you’re going to have a hard time inspiring hence a very shortened and curtailed type of inspiration curve on the bottom half and you also have a curtailed and shortened type of exhalation curve, loop spirometry. So, this would be a good time for you to go back and take a look at your fixed loop spirometry. 02:23 In that particular discussion, we went ahead and talked about two other types of loop spirometries, there were three that were total. We had intrathoracic, extrathoracic. 02:33 At this point, focus on vocal cord dysfunction seen in health care workers. Obstruction of the vocal cords, not in the airways. And CHF and PE may present with wheezing as well, so keep this in mind when you’re dealing with, well, differentials. COPD, well. DLCO. 02:53 Here are the test that you want to do. Vocal cord dysfunction and CHF and PE, some important differentials that you want to keep in mind when dealing with asthma in totality. 03:05 Continuing our differential diagnosis, ABPA stands for Aspergillus bronchopulmonary type of asthma. This is asthma triggered by Aspergillus, and what happens? Kind of behaves like your allergy, what does this mean? Peanut dust, peanut. Specifically here it’s Aspergillus and flavus is the organism that you’re thinking about. Infiltrates on chest x-rays (CXR) and CT, high Aspergillus specific IgE and whenever you’re thinking about IgE then you should thinking about it mounting upon a mast cell and what are you going to release? Very good, histamine. And what kind of effect does histamine have on your bronchi? Bronchospasm. 03:51 Differentials for asthma, keep this in mind. We talked about COPD, I told you about vocal cord dysfunction especially health care workers and then here we’re looking at ABPA. Asthma can be misdiagnosed of many respiratory conditions. So a lot of that wheezing that we’re talking about, keep that in mind that wheezing can be also found in PE as we’ve just discussed.
About the Lecture
The lecture Asthma: Differential Diagnosis by Carlo Raj, MD is from the course Obstructive Lung Disease.
Included Quiz Questions
Which of the following is not on the differential for a patient presenting with suspected asthma?
- Deep vein thrombosis
- Congestive heart failure
- Pulmonary embolism
- COPD
- Allergic bronchopulmonary aspergillosis
Which of the following is not true about aspergillus bronchopulmonary asthma?
- Spirometry diagnostic
- Infectious
- CXR/CT diagnostic
- High Aspergillus specific IgE
- Aspergillus fumigatus most common etiology
Author of lecture Asthma: Differential Diagnosis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Everything has been described so smoothly . I just wanted to know more about classification of asthma.
