Playlist
Show Playlist
Hide Playlist
Adrenal Case: 38-year-old Man with Hypertension

-
Slides 01-02-02 Adrenal Pituitary.pdf
-
Download Lecture Overview
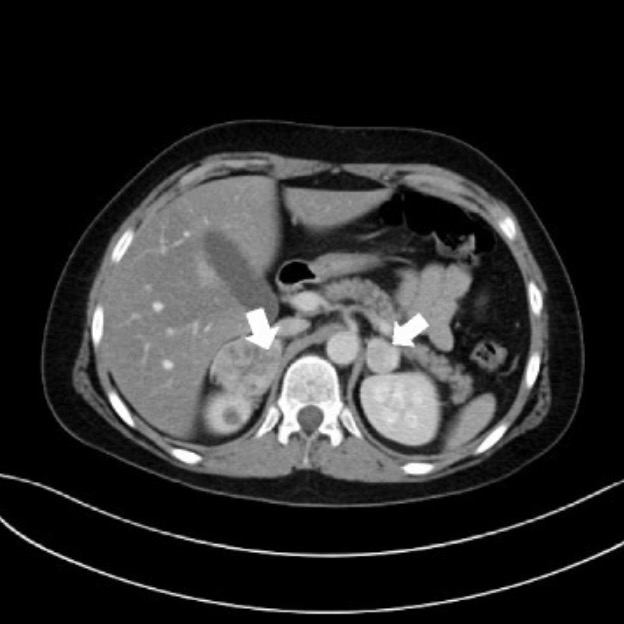
00:00 Let’s go on to another case. 00:03 A 38-year-old man is evaluated for resistant hypertension. 00:07 He was diagnosed with hypertension at age 35 and reported that his blood pressure has never been well-controlled. 00:15 He is compliant with all his medications. 00:18 He denies headaches, chest pain, palpitations, shortness of breath, or symptoms of panic attack. 00:25 He has no history of cardiovascular disease, does not smoke, and does not drink alcohol. 00:30 Medications are lisinopril, amlodipine, hydrochlorothiazide, metoprolol, and potassium chloride supplementation. 00:39 On physical exam, his blood pressure is 155/92. 00:43 His pulse rate is 65 beats per minute. His BMI is 25. 00:48 Examination of the heart is significant for the presence of a fourth heart sound but no murmurs. 00:55 The remainder of the exam is unremarkable. 00:59 Lab studies are significant for a serum creatinine level of 1 mg/dL, a fasting plasma glucose level of 82 mg/dL, and a serum potassium level of 3.2. 01:12 What is the next most appropriate diagnostic step? Here we have a young man with resistant hypertension on three different blood pressure lowering meds. 01:24 Essentially, the definition of resistant hypertension is taking three or more blood pressure lowering meds of which one is a diuretic. 01:33 He also has a low potassium. 01:36 This should trigger the suspicion for primary aldosterone in this patient. 01:40 First of all, the younger onset of his high blood pressure and the degree to which his blood pressure is elevated despite all the medications is enough to make you suspect the condition. 01:54 The conclusion here is that the most appropriate step to perform is to measure the plasma aldosterone to plasma renin activity ratio. 02:03 If this is positive, confirmation testing with IV salt-loading, fludrocortisone suppression testing, or captopril testing should be considered. 02:13 This patient has resistant hypertension defined as a blood pressure that remains above goal despite concurrent use of multiple antihypertensive agents. 02:21 He has significant hypokalemia in the presence of treatment with an ACE inhibitor and potassium supplementation which raises the possibility of primary hyperaldosteronism. 02:34 Adrenal imaging is indicated to determine if hyperaldosteronism is due to a bilateral or unilateral cause. 02:41 Mineralocorticoid receptor antagonists such as spironolactone are indicated for the patients with bilateral causes of primary hyperaldosteronism and those with a unilateral cause who refuse or are not candidates for surgery.
About the Lecture
The lecture Adrenal Case: 38-year-old Man with Hypertension by Michael Lazarus, MD is from the course Adrenal Gland Disorders. It contains the following chapters:
- Adrenal Gland Case: 38-year-old Man with Resistant Hypertension
- Primary Hyperaldosteronism
Included Quiz Questions
Which of the following is indicative of resistant hypertension?
- An elevated blood pressure, despite the concurrent use of 3 or more different antihypertensive agents with at least one being a diuretic
- Chronically elevated blood pressure over 140/90 mm Hg, despite proper lifestyle modifications
- Hypertension in patients older than 35 years of age
- Elevated serum creatinine levels
- BMI greater than 30 kg/m2
Which of the following in combination with hypertension would strongly suggest primary hyperaldosteronism?
- Low serum potassium levels
- High serum chloride levels
- Persistent hypertension despite the use of ACE inhibitors
- Presence of a fourth heart sound
- Low serum sodium levels
Author of lecture Adrenal Case: 38-year-old Man with Hypertension

Michael Lazarus, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
