Playlist
Show Playlist
Hide Playlist
Acute Tubular Necrosis

-
Slides Acute Tubular Necrosis.pdf
-
Download Lecture Overview
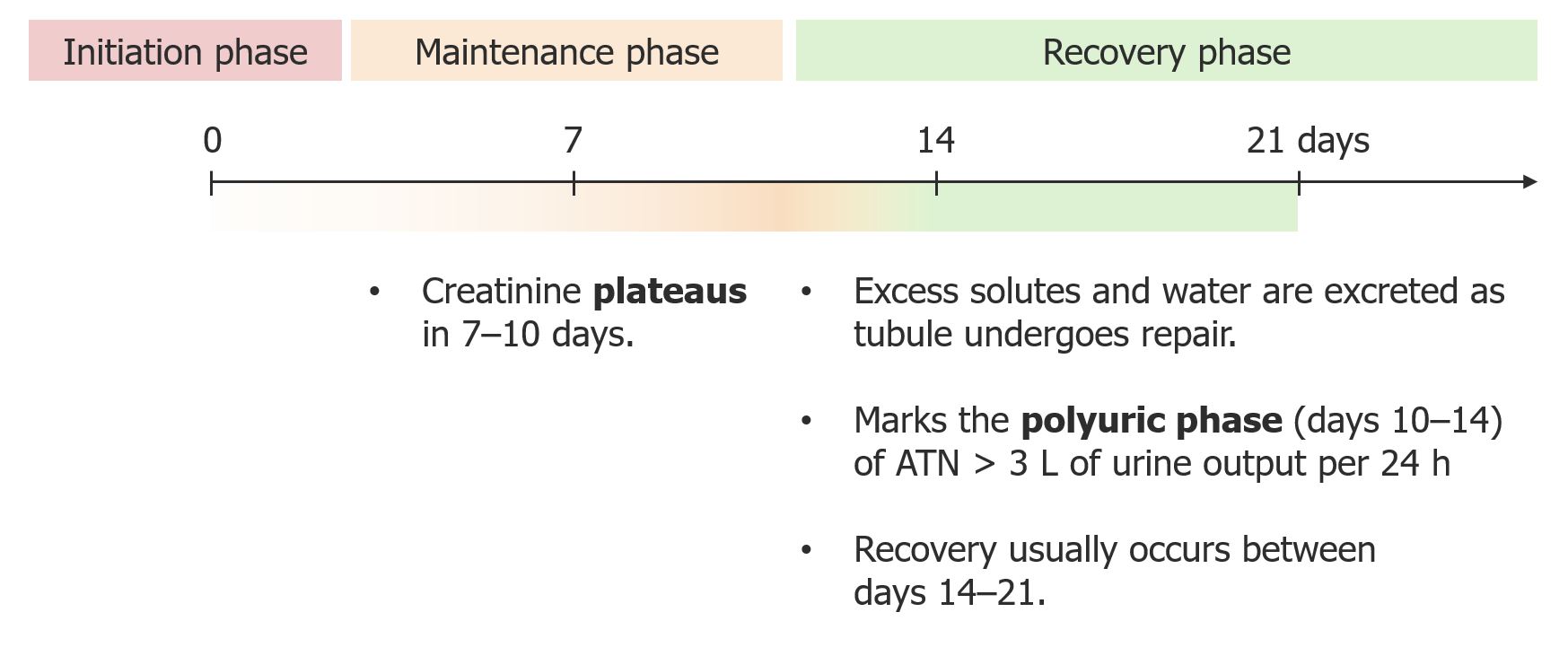
00:01 Acute Tubular Necrosis, ATN, is an extremely important topic to know not only for the USMLE Exam, but also when you are rotating on the wards. 00:11 Now ATN occurs when you have injury to the kidneys from toxins or ischemia resulting in sloughing off of tubular cells into the urine. 00:21 Two of the most common causes of ecai are pre renal disease and 18, which account for around three quarters of AQI cases in the hospital. 00:29 The recovery speed is usually tied to the underlying cause and can range from a few days to several months. 00:35 The mortality rate of this disease can approach 30% with influencing factors including patient age, sepsis, liver failure and ARDS. 00:44 Now very high yield for you to know is that ATN causes granular muddy brown casts into the urine, very important phrase, and this occurs due to detachment of the renal tubular epithelial cells. 00:59 Now the causes of ATN are very important to know and we break them up into different categories: toxins and drug, renal ischemia and crush injury. 01:09 Now for toxins and drugs, these are really important that you know because these are common causes of ATN and you can definitely see it on the wards. 01:18 Aminoglycosides, amphotericin B, cisplatin, foscarnet, radiocontrast dye. 01:25 Whenever you send a patient down for a contrast study, say it’s a CT scan with contrast, you’re always going to be told, check the BUN and creatinine or check the renal function to see are they impaired, at base line or not, because if they are, giving radiocontrast dye will only push them into more renal impairment, so this goes to tell you how much of a potent a flick to radiocontrast dye is to cause ATN. 01:52 Now renal ischemia, this makes sense. 01:56 In settings of sepsis and shock you’re gonna have hypoperfusion to the kidney and acute tubular necrosis will commonly occur. 02:04 In crush injury, when you have crush injury to really any major part of the body, you’re gonna have myoglobulinuria in which myoglobin is released from the crush injury and it naturally causes ATN within the kidney. 02:17 Statin drugs do not directly cause ATN, but they can cause rhabdomyolysis in 1% of patients that take them. 02:24 This rhabdomyolysis can then lead to ATN, in some cases Now like I said, very high yield to know is that in ATN you will see granular muddy brown casts. 02:35 Now these muddy brown cast in ATN are due to renal tubular epithelial cells actually detaching and they can cause occlusion of the renal tubules due to this cast formation which will then increase tubular pressure which will then decrease glomerular filtration rate or GFR and then lead to oliguria. 02:55 Now the clinical course of ATN occurs in three stages and this is really important that you understand in your mind to be able to better understand the path of physiology of the disease. 03:07 The three stages are one, an initiation or inciting event. 03:11 The three stages are one, an initiation or inciting event. 03:12 The second is maintenance or what’s called an oliguric phase and the third is the recovery. 03:17 So for step one of this three stage course, initiation or an inciting event. 03:22 You will have renal tubular cell damage begin due to some type of toxin exposure or ischemia. 03:29 Then the GFR starts to fall and urine output starts to decrease. 03:34 Then you will enter into stage two which is the maintenance stage or also called the oliguric phase. 03:41 Here, renal tubular injury and death is actually established, then GFR is below normal and urine output will be low or even absent and this second stage will last roughly one to two weeks and when you do light microscopy you will see granular casts and you’ll have flattening of tubular epithelial cells and tubular epithelial necrosis. 04:07 And then the third phase is recovery. 04:09 You will have reepithelization of the renal tubes and they will regain their renal function then you’ll have polyuria and gradual normalization of GFR. 04:20 Now people may think, why do we have polyuria? It’s a response to the initial injury, you're making up renal function and this recovery phase takes roughly two to three weeks. 04:32 Now in ATN, the renal tubules become necrotic, very important to know, renal tubules are actually dying and when they sloughed pink epithelial cells and debris and you’ll have loss of nuclear detail. 04:47 Now this can also be the result of rhabdomyolysis by statin use. 04:53 Now myoglobin is released by the muscles when you take statins or from a crush injury and this can cause an increase in CPK levels and these CPK, very important, are toxic to the renal tubular cells especially the proximal tubule.
About the Lecture
The lecture Acute Tubular Necrosis by Mohammad Hajighasemi-Ossareh, MD is from the course Tubulointerstitial Diseases.
Included Quiz Questions
Which of the following urinalysis findings most likely reflects acute tubular necrosis?
- Muddy brown casts
- Hyaline casts
- Fatty casts
- Protein casts
- WBC casts
Which of the following statements is true about acute tubular necrosis?
- The recovery phase is characterized by tubular reepithelialization.
- Creatinine and BUN levels continue to rise in the recovery phase.
- The maintenance phase will last 1–2 months.
- Dialysis is required in approximately 75% of cases.
- An acute rise in the GFR is classic.
Author of lecture Acute Tubular Necrosis

Mohammad Hajighasemi-Ossareh, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
