Playlist
Show Playlist
Hide Playlist
Acute Cholecystitis with Case

-
Slides Gastroenterology 14 LBSD Gallstone Diseases.pdf
-
Download Lecture Overview
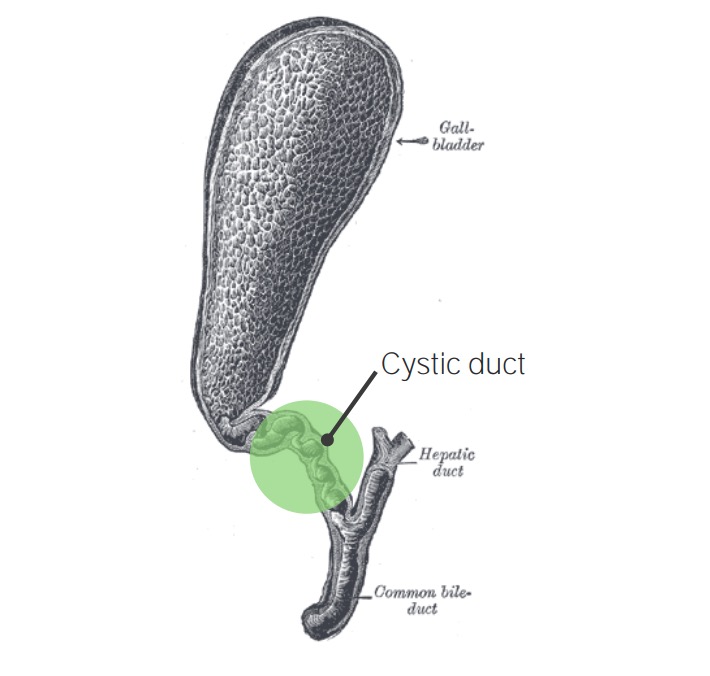
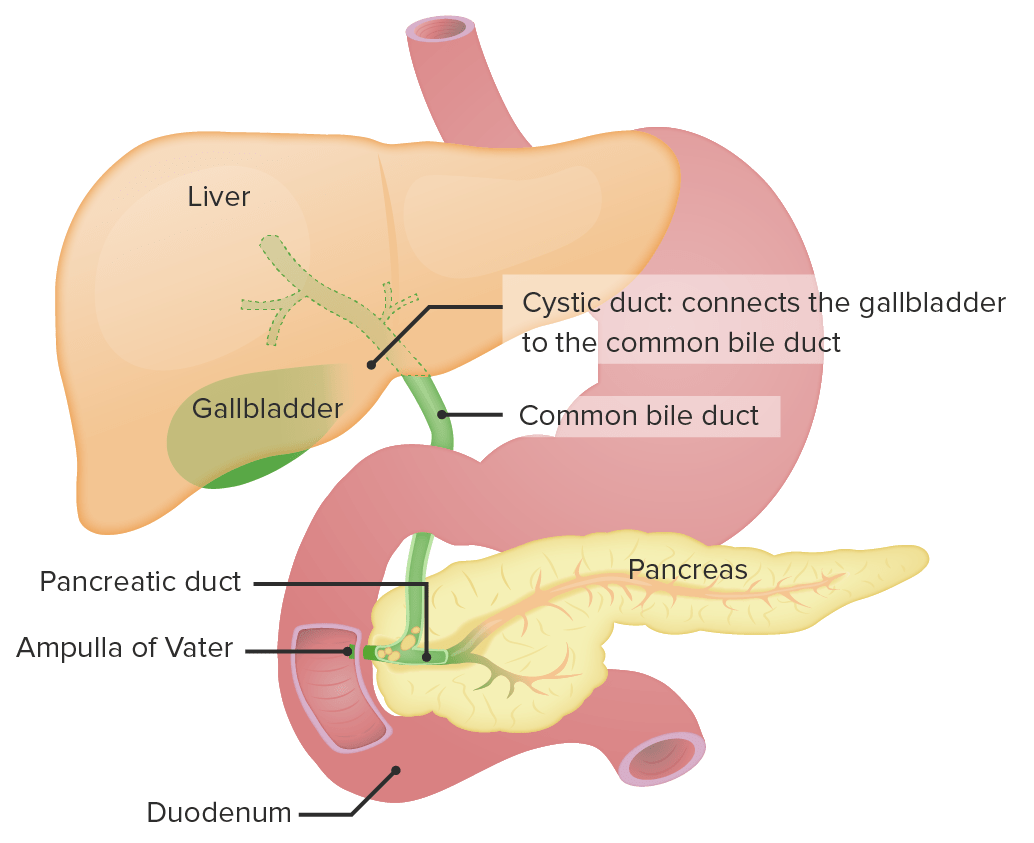
00:01 Let's move to our next case. 00:03 A 31-year-old man with no past medical history presents to the ED with two days of right upper quadrant pain accompanied by fever, nausea and vomiting. 00:14 Over the last few months, he has had intermittent abdominal pain after eating. 00:18 These episodes last for a few minutes then resolve. 00:21 Vitals are notable for temperature of 38.2 C and heart rate of 115 bpm. 00:27 On abdominal exam, he has tenderness to palpation in the right upper quadrant but no rebound or guarding. 00:34 Labs show mild elevation in AST, ALT and the total bilirubin His abdominal ultrasound shows pericholecystic fluid and gallbladder wall thickening. 00:45 So what is the recommended management for this patient? So we'll review this case. 00:51 He has right upper quadrant pain with fever, nausea and vomiting lasting for more than 6 hours and he also has a history of what sounds like biliary colic. 01:03 He has fever and tachycardia. 01:05 On his exam and labs, this helps us localize something to the biliary system And his ultrasound findings are quite concerning. 01:14 So before we answer that question, let's talk about the difference between cholelithiasis or just the presence of gallstones versus acute cholecystitis, which is inflammation of the gallbladder So in cholelithiasis, patients usually present with just biliary colic that tends to be intermittent and self-limited. 01:35 On the other hand, those with inflammation of the gallbladder or cholecystitis will present with persistent pain in the area, fever and may have elevated liver chemistry studies. 01:49 So again, patients with acute cholecystitis tend to present with right upper quadrant pain, fever, nausea and vomiting. 01:58 On physical exam, they will have tenderness in the right upper quadrant and they may have a particular exam finding called "Murphy's sign" This is when you press in on the right upper quadrant and as they inspire or breathe in, this causes the gallbladder to come in contact or move closer to the examiner's fingers, and they will stop breathing in because they experience pain Most cases of of cholecystitis are from obstruction of the cystic duct, which directly drains the gallbladder, via gallstone. 02:31 The diagnosis is made by right upper quadrant ultrasound. 02:35 So some common features that we can discuss here are, you may have fluid surrounding the gallbladder. 02:40 What you would see is a dark or black structure around the surface of the gallbladder You may see gallbladder wall thickening as shown here in that image, the wall is slightly thicker than normal. 02:53 You may see the presence of gallstones or biliary sludge within the gallbladder, as shown here the echogenic or white material within the lumen of the gallbladder. 03:05 And you may also find a sonographic Murphy's sign. 03:08 This is simply the same physical exam finding that we did earlier by pressing on the right upper quadrant and having the patient inspire but in this case is done with the ultrasound probe pressing in on the right upper quadrant. 03:24 So, as a quick aside, we mentioned that 90% of patients with acute cholecystitis are from gallstones. 03:32 But patients may also have no gallstones and develop cholecystitis This is what's called "acalculous cholecystitis", so the absence of stones. 03:43 This usually requires a type of drainage called percutaneous cholecystostomy which we will discuss later. 03:52 So there are some cases when the diagnosis is difficult to make. 03:56 For instance, when you have a high clinical suspicion that your patient has acute cholecystitis based on their presentation but your ultrasound doesn't show those typical findings we discussed. 04:06 In these cases, you may do a special type of scan called a HIDA scan This is also known as cholescintigraphy It is done by injecting a radiotracer that is then taken up by the liver, and then secreted into the biliary tract. 04:24 When we do this, we can look for an obstruction or a blockage anywhere along this path of drainage. 04:31 If after 4 hours, we don't see the gallbladder, then you can suspect either cholecystitis or some type of obstruction of the cystic duct. 04:39 So here's an example shown here where you see the liver light up and eventual drainage into the rest of the system but no gallbladder is seen So, the treatment of acute cholecystitis first involves supportive care so giving IV fluids. 04:58 You then also want to give IV antibiotics to cover your gastrointestinal bacterial flora - so these are gram negative organisms and anaerobes. 05:08 So some choices you may choose are beta-lactam and beta-lactamase inhibitors or a 3rd-generation cephalosporin with metronidazole. 05:19 Next, the patient should undergo a laparoscopic or an open cholecystectomy, so removal of the gallbladder during that same hospital stay. 05:29 If the risk of surgery is too high, you may also do a cholecystostomy drain. 05:35 This is shown here on the right so this involves inserting a needle and then a catheter to drain directly from the skin into the gallbladder. 05:46 So now, we can return to our case. 05:52 We have a 31-year-old man who now has persistent right upper quadrant pain, fever, lasting for longer than 6 hours. 05:56 He has fever and tachycardia. 05:59 His ultrasound findings are concerning and now we know that the presence of pericholecystic fluid and gallbladder wall thickening show us that he has acute cholecystitis. 06:09 So, the recommended management for this patient is to start IV fluids, since he does meet the sepsis criteria. 06:18 Give IV antibiotics and consult surgery for a cholecystectomy.
About the Lecture
The lecture Acute Cholecystitis with Case by Kelley Chuang, MD is from the course Disorders of the Hepatobiliary Tract.
Included Quiz Questions
Which of the following is the best next step in the diagnosis of cholecystitis if the ultrasound examination findings are equivocal?
- HIDA scan
- Abdominal CT
- Abdominal X-ray
- MRCP
- ERCP
Which of the following is more characteristic of cholelithiasis than cholecystitis?
- Intermittent and self-limited RUQ pain
- Persistent RUQ pain
- Fever
- Murphy sign
- Elevated values on liver chemistry studies
Which of the following is the diagnostic test of choice for cholecystitis?
- Abdominal ultrasonography
- HIDA scan
- MRCP
- Abdominal CT
- Abdominal X-ray
Author of lecture Acute Cholecystitis with Case

Kelley Chuang, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Exceptional acumen in anticipating difficulties and nuances in learning the different concepts involving biliary pathology.
really well explained. simple and informative, not too complicated. management helpful
