Playlist
Show Playlist
Hide Playlist
Abnormal Placentation


-
Slides Abnormal Placentation Obstetrics.pdf
-
Download Lecture Overview
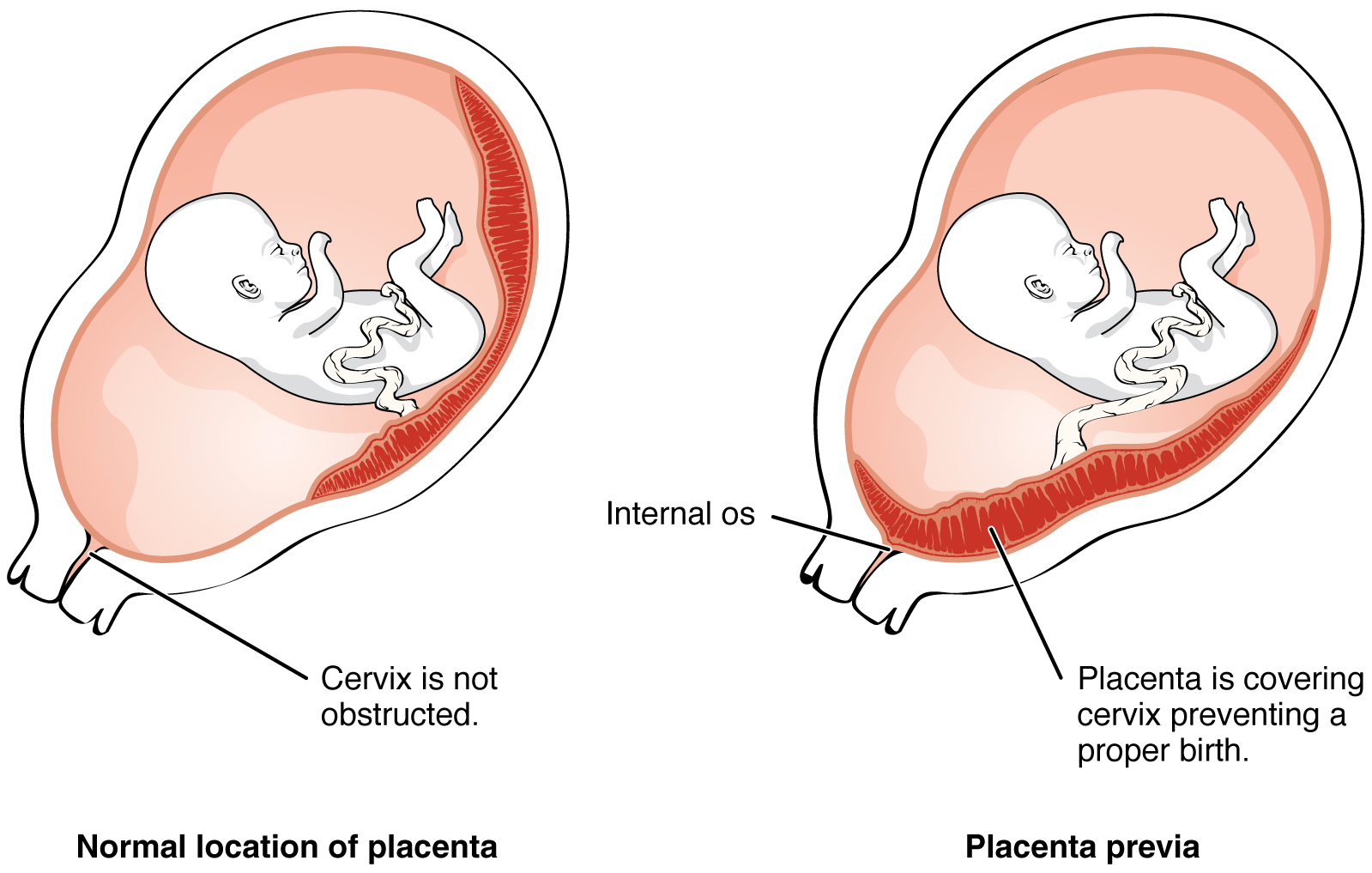
00:01 Let's discuss placental abnormalities. 00:04 Before we discuss what's abnormal, let's discuss what normal placenta looks like. 00:09 When we talk about the anatomy of normal placenta, we notice the placenta disc and that's divided into the basil plate, which is the maternal side of the placenta, and the chorionic plate - that's the fetal side of the placenta as you can see here. 00:22 We have the membranes and then we have a three-vessel umbilical cord. 00:25 Now, unlike the other structures in the human body, this three-vessel cord has two arteries and one vein. 00:33 Now let's talk about some of the placental structural abnormalities. 00:37 First, let's talk about a succenturiate lobe. 00:41 So this abnormality is one in which an extra lobe separates from the placenta. 00:47 The clinical manifestation of this can be postpartum hemorrhage. 00:51 At times that extra lobe can separate and when you're delivering the placenta, that extra lobe does not come out, and it can be a cause of postpartum hemorrhage because of retained products. 01:03 Next, let's talk about a velamentous insertion. 01:07 So with the velamentous insertion, the umbilical vessels traverse the membranes as you can see here. 01:14 The vessels are easily compressible and so that's the clinical manifestation. 01:19 Also, it can be associated with placenta previa. 01:24 Vasa previa. 01:27 So with vasa previa, the vessels traverse the cervical os. 01:30 So you can see here in the picture, that the vessels are in front of the fetal head. 01:35 Now that can be problematic. 01:36 If those vessels are lacerated during a cervical exam, or artificial rupture of membranes, the baby can exsanguinate. 01:43 So it's important to know if the patient has a vasa previa prior to delivery. 01:50 Let's go through a question about abnormal placentation. 01:53 A patient is known to have a velamentous insertion, what is the most likely fetal abnormality to be seen on fetal heart rate tracing while in labor? A. Late decelerations, B. Recurrent variable decelerations, C. End stage bradycardia or D. recurrent accelerations Well, the answer is recurrent variable decelerations. 02:15 Remember those vessels are easily compressed and when we have compression of vessels, that causes recurrent variable decelerations. 02:25 Now that we've talked about abnormal placental structure, now let's talk about abnormal placenta location. 02:32 So we have placenta previa, placenta accreta, placenta increta, or placenta percreta. 02:39 Let's start with placenta previa. 02:41 So this is a situation in which the placenta is located near or over the cervical os. 02:48 If disrupted in pregnancy, it can cause significant antepartum hemorrhage. 02:52 It can actually cause death of the baby. 02:55 And C-section is usually the recommended route of delivery. 02:58 You can imagine if the placenta is covering the cervix, then the fetus is not able to come through that through the cervical os. 03:06 Now, placenta accreta. 03:09 So with placenta accreta, the placental trophoblast invade to the myometrium. 03:15 On histology, we noticed an absence of Nitabuch’s layer , that's how we diagnose it. 03:21 It can be associated with placenta previa, and the placenta can be very difficult to remove at the time of delivery, that can make this a cause of postpartum hemorrhage because of retained products of conception. 03:35 Now increta, placenta increta is a condition in which the placenta trophoblast invade through the myometrium. 03:43 Remember, accreta was just to the myometrium, now we're talking about through the myometrium. 03:49 It can also be associated with placenta previa, just as accreta can, and the placenta is usually very adherent during delivery and this can be a cause of postpartum hemorrhage. 03:59 Usually, C-section with hysterectomy is the management option, because we're unable to physically remove the placenta so the whole uterus has to be removed. 04:10 Now percreta. 04:13 In placenta percreta, the placental trophoblast are through the serosa. 04:17 So remember with accreta, we were 'to' the myometrium, with increta, we were 'through' the myometrium and percreta, we are completely through the myometrium and through the serosa, so now we're going outside of the uterus. 04:30 The placental tissue can be in various places outside of the uterus, most commonly the bladder or the rectum, and this causes severe hemorrhage at the time of delivery. 04:40 Because of this, we don't try to remove the placenta. 04:43 And you can imagine, we can't remove the placenta if it's into the bladder, or if it's to the rectum. 04:48 And so a lot of times we do C-section with hysterectomy, and we leave some of the placenta in situ. 04:53 Again, we can't remove it from the bladder or the rectum if it has invaded that far. 05:00 So let's talk about another question. 05:03 What ultrasound finding is seen in placenta accreta? Is it A. lambda sign? Is it B. absence of Nitabuch's layer? C. the double peak sign or D. a Tri laminar layer? Do you remember this from the lecture? That's right, the answer is B - absence of Nitabuch's layer.
About the Lecture
The lecture Abnormal Placentation by Veronica Gillispie, MD, MAS, FACOG is from the course Antenatal Care. It contains the following chapters:
- Placenta
- Abnormal Placenta Presentation
- Abnormal Placental Location
Included Quiz Questions
Which of the following can be a potential cause of recurrent variable decelerations noted on fetal heart tracing during labor?
- Velamentous cord insertion
- Succenturiate placental lobe
- Vasa previa
- Placenta increta
- Placenta previa
Which of the following is the recommended route of delivery for placenta previa?
- Cesarean section
- Cesarean section and hysterectomy
- Normal vaginal delivery of fetus and placenta
- Normal vaginal delivery of fetus followed by operative delivery of the placenta
- Induction of labor at 35 weeks gestation
Which of the following is the appropriate mode of delivery for a patient with placenta increta?
- Delivery by cesarean section followed by hysterectomy
- Delivery by cesarean section without hysterectomy
- Normal vaginal delivery followed by hysterectomy
- Normal vaginal delivery
- Normal vaginal delivery followed by operative delivery of the placenta
Which of the following conditions is best described as placental tissue invading through both the myometrium and serosa of the uterus?
- Placenta percreta
- Placenta increta
- Placenta accreta
- Placenta previa
- Placental abruption
Author of lecture Abnormal Placentation

Veronica Gillispie, MD, MAS, FACOG
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
