Playlist
Show Playlist
Hide Playlist
Open Pneumothorax & Flail Chest

-
Emergency Medicine Pulmonary Trauma.pdf
-
Download Lecture Overview
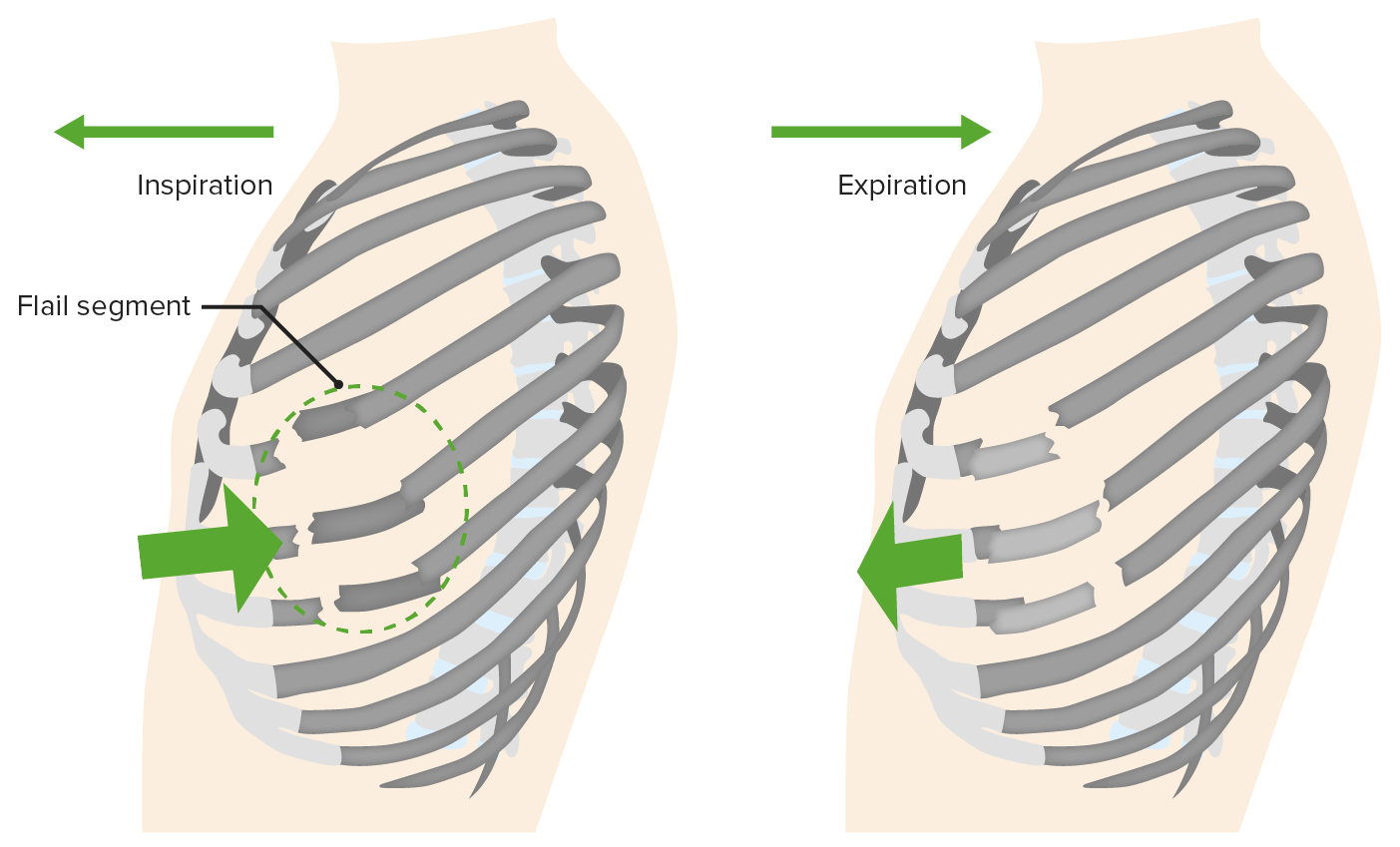
00:01 Alright, now we’re gonna move on to some other pulmonary life threats. 00:05 The next one is open pneumothorax. 00:07 So open pneumothorax is kind of interesting physiologically. 00:11 This happens when you have a large, open defect in the chest wall and if we all remember our fluid flow physics, when you have a tube and you’re trying to determine the rate of flow through that tube the primary determinant of flow is gonna be the radius of the tube and then the second most important determinant is the length. 00:34 So if you think about your trachea as a tube and you think about the hole in your chest wall as a tube, you can imagine the chest wall is much shorter too, right? It’s a lot smaller than the trachea so when that wound goes up to 2/3 of the tracheal diameter, it doesn’t have to be the size of the trachea or bigger than the trachea, it can still be smaller because the tube is so much shorter. 00:58 When that happens inspiration is gonna preferentially pull air through the wound into the pleural space rather than going down the trachea and into the lungs. 01:10 So if you have a large enough defect here, you’re not gonna pull air through the bronchial tree the way you’re supposed to, you’re gonna pull air in directly through the wound when you breathe. 01:22 Now as you can imagine, if you’re just sucking air into your pleural space through a hole in your chest, that’s gonna render your ventilation pretty ineffective so this can result in lethal hypoxia and respiratory failure if it’s not treated promptly. 01:36 So again, large wound in the chest wall on physical exam, anything bigger than 2/3 the size of the trachea is gonna cause air to preferentially flow into the wound. 01:48 This is also known as a sucking chest wound and that’s because these wounds make a delightful sucking sound during the respiratory cycle. 01:55 You can actually hear air being pulled in through the wound and it goes [sucking sound] with every respiratory effort. 02:04 It’s gonna cause hypoxia and respiratory distress and you don’t need radiologic confirmation for this. 02:10 You can actually see the wound, you can hear the sucking sound, you can appreciate the patient’s respiratory distress, you’re gonna go ahead and treat it. 02:17 So the treatment is very satisfyingly simple. 02:21 You basically just place an occlusive dressing over the wound and what’s gonna happen when you do that is when the patient breathes in, now you’ve got the hole occluded so it’s gonna suck the dressing up against the chest wall but it’s not gonna let any air go through the wound. 02:37 Well, if air can’t get through the wound, where is it gonna go? Now it’s gonna go down through the trachea into the bronchial tree where it belongs. 02:45 However, we wanna make sure that we allow air to escape from this wound during exhalation because you don’t know what kind of injury there is to the underlying lung and you don’t wanna create a tension pneumothorax so the way we do this is by securing the occlusive dressing only on 3 sides and that creates a one-way valve effect. 03:06 So when the patient breathes in no air goes through the wound, but when they breather out air can escape out through the wound if it needs to and that’s gonna prevent the development of a tension Pneumothorax. 03:20 These patients always need chest tube for definitive management. 03:24 Again, the lungs not gonna be able to re-expand and heal unless you restore the negative intrathoracic pressure which is accomplished with a chest tube and there is a high incidence of underlying injury. 03:35 You can imagine that any kind of traumatic mechanism that makes a big hole in your chest wall is gonna be very likely to be associated with other pathology, so these patients often end up going to the operating room for other reasons. 03:49 Alright, next pulmonary life threat to talk about is flail chest. 03:52 A flail chest occurs when you have multiple rib fractures. 03:56 So basically, if you have multiple fractures of ribs that are adjacent to one another and the fractures are present in two different locations, you get a section of rib that is discontinuous from the rest of the thoracic cage. 04:12 Well, what’s gonna happen to that section of rib? It’s not tethered down to the other ribs now so it’s not gonna move normally during the respiratory cycle, it’s gonna actually move paradoxically. 04:24 So normally, when you breathe in your ribs follow that bucket handle motion and sort of expand, but now you’ve got a section of chest wall that’s not gonna do that, it’s gonna go [sucking sound] and suck up against the lung during inspiration. 04:39 This is gonna directly impair ventilation because now you have a section of rib that’s floating around doing its own thing and it’s gonna also be strongly associated with underlying pulmonary contusion because the section of rib, one, it got broken somehow so clearly there’s gonna be a high likelihood of transmission of energy to the underlying lung and two, you were repeatedly injuring the lung by pulling the section of rib up against it over and over again. 05:10 So patients with flail chest you’re gonna be able to physically see a chest wall deformity on your clinical exam. 05:17 This is not gonna be a subtle finding. 05:19 You’re gonna see that paradoxical chest wall movement in the area of affected rib. 05:24 You’re gonna see infiltrates on your chest x-ray which are suggestive of underlying pulmonary contusion and the treatment for this in the ED is really gonna be supportive. 05:33 We’re gonna wanna make sure that we provide the patient with supplemental oxygen, that we maintain their oxygenation, that we intubate and mechanically ventilate them if they are in significant respiratory distress, but there’s not really any definitive treatment that we can offer for this in the ED setting. 05:51 In many cases, these patients with supportive care will just go on to heal their rib fractures and be fine although there are situations where surgical fixation of the chest wall might be necessary.
About the Lecture
The lecture Open Pneumothorax & Flail Chest by Julianna Jung, MD, FACEP is from the course Trauma (Emergency Medicine). It contains the following chapters:
- Open Pneumothorax
- Flail Chest
Included Quiz Questions
What is the definitive management for open pneumothorax?
- Chest tube placement
- Occlusive dressing
- Positive pressure ventilation
- Orotracheal intubation
- Oxygen supplementation
What causes flail chest?
- Fracture of multiple adjacent ribs in two locations
- Large open wound in chest wall
- Progressive build-up of air inside the pleural cavity
- Collapse of one lung
- Rupture of pleural blebs
Which of the following statements regarding flail chest is INCORRECT?
- The definitive management is placement of a chest tube.
- It is associated with pulmonary contusion.
- It is observed as a paradoxical movement of the chest wall.
- Infiltrates can be seen on the chest radiograph.
- Flail chest directly impairs ventilation.
Author of lecture Open Pneumothorax & Flail Chest

Julianna Jung, MD, FACEP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Thank you for your lectures. They are very easy to follow and interesting to watch.
