Playlist
Show Playlist
Hide Playlist
Bradycardia: Sinus Bradycardia and Heart Blocks



-
Slides Bradyarrhythmia CardiovascularPathology.pdf
-
Download Lecture Overview
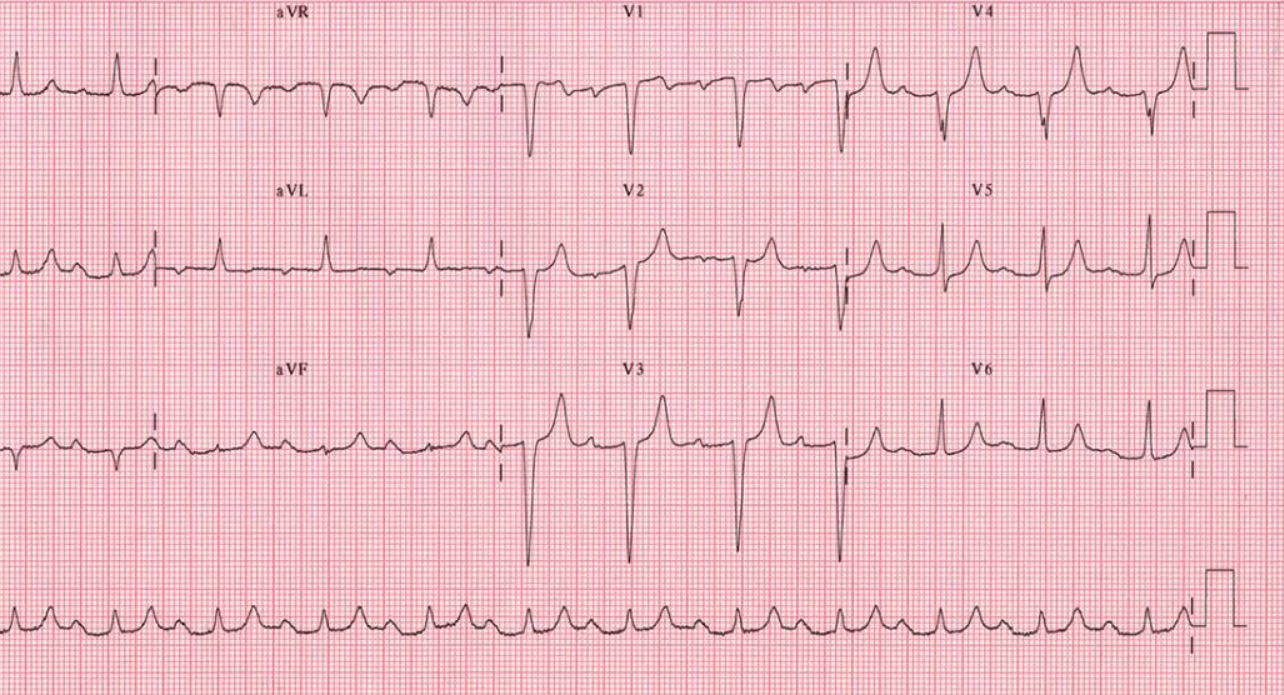
00:01 So with arrythmias. We said there was two major categories. 00:05 One was one in which it was conduction system diseases, and then the vascular component. 00:12 Now, what we will first discuss would be the conduction system disease category first, and our first topic under this would be bradyarrhythmia. 00:22 So, what is brady? Well, I told you earlier that if you find your beats per minute, which is normally 60-100, to be less than 60, and trust me, you'll know if your patient has decreased heart rate. 00:39 Now, sinus bradycardia, what does that mean to you? It means that the R wave, and you compare one R wave to another, are further apart. 00:47 And earlier, I told you -- it's sounds like a "telephone number," which is your 300-150-100. So, what exactly does that mean? Well, when you look at that ECG, if there's only one line separating an R wave from each other, that is 300 beats per minute, okay? What if there's two lines separating an R wave? 150. 01:16 Three lines, 100. You group those together, 300-150-100, stop. 01:23 Just like a phone number, you divide that into whatever numbers so that you can remember this easily. 01:30 The other three numbers were 75, 60, and 50. 01:35 So, if 60 brings you to six lines separating an R wave from one another, that's 60 beats per minute. Welcome to bradycardia, and sinus means what to you? Sinoatrial wave representing the existence of a P wave. 01:53 Is that clear? Now, can be seen in competitive athletes. 01:58 It's perfectly normal and that you can expect. 02:01 So, if you take a look at the R waves, that is the upper deflection here, and you find a number of lines in between them, well, you're in the realm of bradycardia. 02:10 Now, with competitive athletes, there's one more thing that I wish to bring to your attention. 02:15 Apart from having a normal sinus bradycardia, you can also have a patient who's an athlete that has a well-trained and very efficient left ventricle, right? What does that bring -- what are you referring to? Well, I'm referring to the fact that with a very efficient left ventricle that could be enlarged, but you have proper cardiac output, you might hear what heart sound? Granted. S1 and S2. You have to, right? If the person's alive. But it's the S3 that I'm really having you pay attention to. 02:52 S3 would be fine in that patient and we have discussed that earlier. 02:56 If symptomatic in older patients, well, syncope is what you're worried about. 03:01 So now, let's get into our clinical manifestation. So, could it be normal? Sure. 03:06 Competitive athletes, marathon runners, well-conditioned individuals, right? But you can also have symptomatic in -- if you have an older patient that has sinus bradycardia, that means that perhaps this patient might not have enough cardiac output. 03:20 Uh-oh. If there's not enough cardiac output, then the patient may be suffering from syncope. 03:25 That is not very good. Not a good feeling. 03:28 And treated with what? A permanent pacemaker. All right? Now, heart block is where we go next. 03:37 So, sinus bradycardia, I gave you two differentials there, a competitive athlete and an older patient in which, unfortunately, they're just sinus brady and may require pacemaker, okay? But if it's a heart block, what does that mean to you? It's not that a conduction is -- or an impulse is not travelling through at all. 03:54 Are you with me? So, the impulse will be travelling through, but it might be retarded, it might be delayed. 04:01 At some point in time, when the heart block gets bad enough and it doesn't travel through at all, guess what degree we're in now? A third-degree AV block. Okay? Now, the same concept was also used for LBBB and RBBB, which are a bundle branch block. 04:19 You call it a block, but the impulse is still travelling through, at a very slow rate. 04:26 Let's talk about heart block. First-degree, second-degree, third-degree. 04:33 Under second-degree, we will then gen into Mobitz type 1 and Mobitz type 2. 04:39 At least know that before you walk into any medical environment. 04:44 Third-degree, that is a complete heart block. Okay? Now, a couple of -- obviously, I have to talk about physio here and some of the fundamentals that we already laid down are for ECG. 04:57 So, what was the name of the -- what would you -- what interval would you name this if I was to describe you -- describe to you the impulse that originated in the SA node making its way down into AV node. 05:11 What interval would you define that as being? PR interval? Good. 05:15 Can you tell me what the time is, normally? 0.12 seconds to 0.2 seconds. 05:21 Do you remember that? Good. So now, you start having issues with a delayed impulse. 05:27 What can you expect that PR interval to do? Good. Increase. 05:33 It'll be greater than 0.2, that's what you're paying attention to. 05:36 So far, so good. Now, is that in every single case? No, and you'll see why. Okay? You'll see conditions in which you won't always find a PR interval, but still will be defined as being a type of heart block. 05:49 You see what I'm referring to. 05:50 Now, the second part of this so that it will make sense to you is, say that you did have a third degree AV block, okay? And if you did have a third-degree AV block maybe because of myocardial infarction. 06:01 There is no impulse that is being dictated by your SA node. 06:05 Now remember, the SA node is the conductor of the heart. 06:09 It is the Zubin Mehta of your conduction of a symphony. 06:13 And so therefore, if the SA node loses control, how? With the third-degree AV block, then who's controlling your ventricles? And ectopic foci. What does that mean? Every single part of the heart is its own pacemaker, right? But you have to have a ring leader. That's your SA node. 06:33 And if that SA node loses the control of the conduction system of the heart, trust me, the heart itself has an inherent ability of creating an ectopic foci. All right? Now, that ectopic foci may still cause contraction of left ventricle or create electrical activity, but it doesn't look normal. You tell me. 06:56 What is the ventricular depolarization represented as an ECG? QRS complex. 07:03 Are you picturing that? Now, say that it's an ectopic foci. 07:07 The QRS complex it looks bizarre. 07:10 There's going to be no correlation between the P wave and the QRS complex. 07:16 So, these are the things that you wanna lay down before you even move forward with any one of these, so that when we get to the topic at hand, we'll be able to go through it efficiently.
About the Lecture
The lecture Bradycardia: Sinus Bradycardia and Heart Blocks by Carlo Raj, MD is from the course Arrhythmias: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following values of heart rate define sinus bradycardia?
- <60 beats/minute
- >60 beats/minute
- <40 beats/minute
- <50 beats/minute
- <70 beats/minute
Which of the following scenarios involves sinus bradycardia as a physiological adaptation?
- Well-conditioned athletes
- Renal failure
- Heart failure
- Atherosclerosis
- Left ventricular hypertrophy
What is the most common symptom associated with symptomatic sinus bradycardia?
- Syncope
- Dyspnea
- Hypertension
- Headache
- Chest pain
Author of lecture Bradycardia: Sinus Bradycardia and Heart Blocks

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
very good intro to heart blocks. I think next few lectues would also help if details are provided.
