Playlist
Show Playlist
Hide Playlist
Sexually Transmitted Infections: Drips/Discharges, Pelvic Inflammatory Disease, and Trichomonas Vaginalis

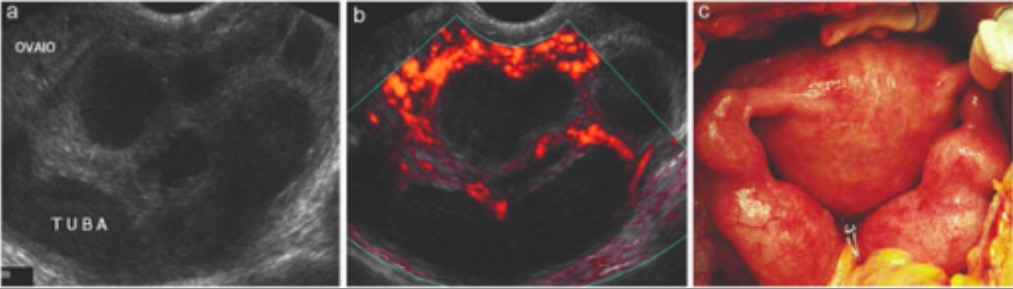

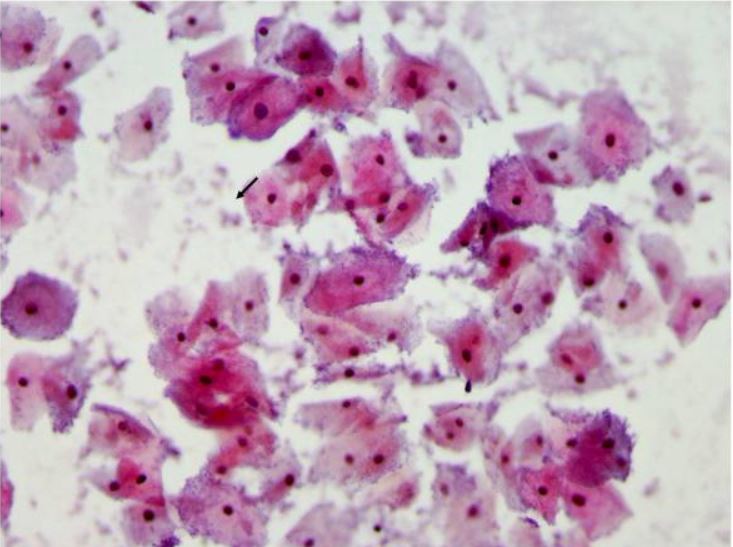
00:01 Let's now review another case. 00:03 A 35 year old woman who is HIV-positive presents with a one week history of yellow vaginal discharge and mild dysuria. 00:11 What about her HIV status concerns you? I'll let you think about that. 00:25 Well, what's in your differential diagnosis? What would you do next? If you're taught to ask the patient, "is she using condoms during sex?" That's a good question. 00:38 You want to ask every patient, "Do you use barrier contraception to avoid STIs?" But especially in HIV-positive patient as she can transmit the virus to her partner. 00:49 Offer the patient testing for her partner in case she does have a partner. 00:55 Could she possibly have an STI? Well, she does have an abnormal discharge. 01:01 You also wanna ask the patient, is she taking her HIV meds? this is important as it keeps the virus titers low. 01:09 Typically, patients are treated with anti-retrovirals. 01:13 What else should she be screened for? Let's go on as you think about that. 01:20 Well, let's now talk about the second criteria for the CDC's diagnosis of clinical drips. 01:27 So, gonorrhea is a very common cause of a discharge in a woman. 01:33 You can also have nongonococcal urethritis, chlamydia, mucopurulent cervicitis and trichomonas vaginalis that causes vaginitis and urethritis and of course, bacterial vaginosis. 01:48 Remember that bacterial vaginosis is not an STI but it is sexually associated and let's not discuss that now. 01:56 The vagina typically has an acidic ph but with intercourse, the sperm increases the ph of the vagina and actually causes an overgrowth of certain bacteria. 02:07 This leads to a fishy, vaginal discharge that these patients can suffer from recurrently. 02:16 Let's now talk about gonorrhea. 02:18 Gonorrhea is a urogenital infection in the female and can cause infection specifically in the endocervical canal. 02:26 70 to 90% also colonize the urethra. 02:30 The incubation period is unclear but usually signs and symptoms occur within ten days of an infection. 02:37 Most patients complain of a vaginal discharge, painful urination or dysuria and labial pain, swelling or abdominal pain. 02:45 There are other forms of urethritis besides those caused by gonorrhea. 02:50 They can be nongonococcal urethritis. 02:53 20 to 40% actually is caused by chlamydia. 02:57 Another 20 to 30% is caused by mycoplasma, another half is actually unknown. 03:05 And occassionally, trichomonas vaginalis and HSV can cause urethritis. 03:11 You can have mild dysuria or pain upon urination and sometimes a vaginal discharge that is mucoid. 03:19 You can see polymorphonuclear cells on a urethral smear. 03:24 but that's typically very painful and hard to tolerate. 03:28 You can see on microscopy in the urine that there would be the presence of white blood cells and you may see the presence of leukocyte esterase. 03:38 Let's now talk about chlamydia. 03:40 Chlamydia can mostly be asymptomatic. 03:43 It's actually asymptomatic but causes a lot of morbidity especially to the female GYN tract. 03:50 Clinical manifestations of chlamydia include cervicitis, urethritis and PID. 03:56 PID can be very devastating to a woman's fertility. 04:00 Complications include potential transmission to a newborn during delivery. 04:05 This can cause conjunctivitis and pneumonia in a newborn and the pediatricians need to be alerted to the status of mom if she has chlamydia. 04:16 Let's now look at what a normal cervix looks like. 04:19 Here you can see the cervix is pink and looks to have no discharge or lesion. 04:24 However, this cervix appears intensely red and angry and has a discharge. 04:31 So typically, when you wanna test for chlamydia, you would insert a Q-tip that allows us to obtain some of the mucus and send that off for PCR or nucleic acid testing. 04:46 You can also do a gram stain to look for gonorrhea. 04:52 You can do a non-culture, non-amplified test or you can do a nucleic acid amplification test and you can use urine, cervical swabs as I just described, urethral swabs, vaginal swabs and also a PAP smear. 05:09 But we typically don't use a PAP smear to screen for STIs. 05:14 And don't forget, you can do serology especially when you have LGV present. 05:20 Let's now just briefly go over the treatment. 05:23 I don't think this will be on your exam, but in case you wanna know more information, just quickly look through this slide. 05:30 If you have gonorrhea, it's recommended that you have IM ceftriaxone. 05:35 And you should also be treated for a co-infection with chlamydia even if you tested negative. 05:40 This includes azithromycin and doxycycline. 05:45 If you have chlamydia, you can just take azithromycin or doxycycline. 05:50 As an alternative, you can take erythromycin, levofloxacin or other medications such as ofloxacin. 06:01 Let's now review PID. 06:04 10 to 20% of women who have gonorrhea and chlamydia actually develop PID. 06:10 In north America, there is a high proportion of chlamydia than gonorrhea in patients who have PID symptoms. 06:18 Let's now review the CDC minimal criteria. 06:21 You may have uterine tenderness, adnexal tenderness or you may have cervical motion tenderness. 06:28 Remember that the adnexa is a zip code, not an address. 06:32 There are many things that live in the adnexa including the ovaries and the fallopian tubes. 06:37 However, we also have bowel and also sometimes the ureter. 06:44 Other symptoms include: endocervical discharge, fever, lower abdominal pain. 06:50 And the complications result in infertility. 06:53 With one episode of PID, you could have a rate of 15- 24% of infertility secondary to gonorrhea or chlamydia. 07:01 You have an increased risk of ectopic pregnancy with just one episode of PID. 07:07 And of course, chronic pelvic pain is increased in the population who has suffered from PID. 07:13 Prevention is best. 07:16 Let's now talk about some of the pathologic findings that you see upon laparoscopy. 07:22 This may not be too clear here but this is a laparoscopic picture what we would look up at the liver and see that there are adhesions forming from the anterior abdominal wall to the liver. 07:35 This is called Fitz-Hugh Curtis syndrome. 07:37 It look like violin strings and if you see this, this is pretty much confirms that the patient has had PID. 07:47 Also, if a patient becomes pregnant after PID, remember that her ectopic pregnancy risk is increased seven times after a single incidence of PID. 07:58 And ectopic pregnancy is a medical emergency and can be potentially fatal if not promptly diagnosed and managed. 08:07 Let's now talk about the outpatient treatment of PID. 08:11 Again, I don't think this will be on your exam but it's helpful to know as you start rounding on the wards. 08:18 What's recommended is ceftriaxone plus doxycycline plus metronidazole. 08:23 There are other combinations as well. 08:26 Please download the slide for more information. 08:30 Let's now talk about Trichomonas vaginalis. 08:33 This is a sexually transmitted parasite. 08:36 There are lots of cases worldwide. 08:39 This is from a figure from the WHO and it had been almost 250 million new cases. 08:46 This occurs in about 3.1% of the US female population but don't forget we have a large immigrant population in the US and can be higher in those who do not originate from the US. 08:59 The prevalence of trichomonas actually increases with age and the highest rates are in African-American women. 09:05 We find trichomonas in 2.5 to 23.2% of adolescents. 09:12 And we also find a higher prevalence in women who abuse drugs at 8.6 to 38%. 09:19 This is what you might see upon speculum examination. 09:23 Here you see a cervix that has a copious discharge. 09:27 It may not always be colored but it can be yellow or white and sometimes appear as frothy but that varies and is difficult to ascertain. 09:38 Let's now talk about the treatment. 09:40 Again, I don't think this will be on your test, but just know for the boards and the wards that metronidazole is the primary treatment. 09:49 There are alternatives such as tinidazole. 09:54 Remember that metronidazole is the preferred agent in women who are HIV infected. 10:02 Thank you for listening and good luck on your exam.
About the Lecture
The lecture Sexually Transmitted Infections: Drips/Discharges, Pelvic Inflammatory Disease, and Trichomonas Vaginalis by Lynae Brayboy, MD is from the course Gynecologic Pathology: Infections, Neoplasms and Screening. It contains the following chapters:
- Case Study and Drips/Discharges: Gonorrhea, Nongonococcal Urethritis and Chlamydia
- Pelvic Infammatory Disease (PID)
- Trichomonas Vaginalis
Included Quiz Questions
Which of the following is the primary site of infection of gonorrhea?
- Endocervical canal
- Ovary
- Fallopian tube
- Vagina
- Endometrium
A two-week-old neonate is brought to the clinic by the mother who explains that her child is wheezing. Upon examination, the infant is afebrile with a wheeze and staccato cough. The lungs are tympanitic to percussion and the eyes appear crusty bilaterally. A Gram stain of the crust is negative for bacteria but shows neutrophils. Which of the following organisms could be responsible?
- Chlamydia trachomatis
- Neisseria gonnorhea
- HIV
- Trichomonas vaginalis
- Herpes simplex
Which of the following is NOT commonly a sensitive test to identify Chlamydia trachomatis?
- PAP smear testing
- Culture
- Nucleic acid amplification test
- Non-culture and non-amplified tests
- Serology
Which of the following is the recommended treatment for non-gonococcal urethritis?
- Azithromycin 1 gm PO X 1
- Erythromycin base 500 mg PO QID X 7 days
- Erythromycin base EES 800mg po QID X 7 days
- Levofloxacin 250mg po qd X 7 days
- Ofloxacin 300mg po BID X 7 days
Which of the following is NOT a complication associated with pelvic inflammatory disease?
- Endometriosis
- Infertility
- Chronic pelvic pain
- Ectopic pregnancy
- Tubo-ovarian abscess
Which of the following best describes the adhesions in Fitz - Hugh - Curtis syndrome?
- Adhesions from anterior abdominal wall to the liver
- Adhesions from anterior abdominal wall to the spleen
- Adhesions from anterior abdominal wall to the pancreas
- Adhesions from anterior abdominal wall to the colon
- Adhesions from anterior abdominal wall to the urinary bladder
Which of the following is a recommended treatment of choice for outpatient treatment of pelvic inflammatory disease?
- Ceftriaxone + doxycycline + metronidazole
- Ceftriaxone + ciprofloxacin + metronidazole
- Cefexime + doxycycline + metronidazole
- Ceftriaxone + ampicillin + metronidazole
- Cefotaxime + doxycycline + metronidazole
Which of the following is the recommended treatment of choice for outpatient treatment of pelvic trichomonas vaginalis?
- Metronidazole
- Ciprofloxacin
- Ampicillin
- Ceftriaxone
- Azithromycin
Author of lecture Sexually Transmitted Infections: Drips/Discharges, Pelvic Inflammatory Disease, and Trichomonas Vaginalis

Lynae Brayboy, MD
Customer reviews
3,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
0 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
The lecture is well organised and the facts are explained clearly. I just think the lecture could be more detailed than it is.
