Playlist
Show Playlist
Hide Playlist
Pulmonary Embolism (PE): Management

-
Emergency Medicine Bord Pulmonary Embolus.pdf
-
Download Lecture Overview
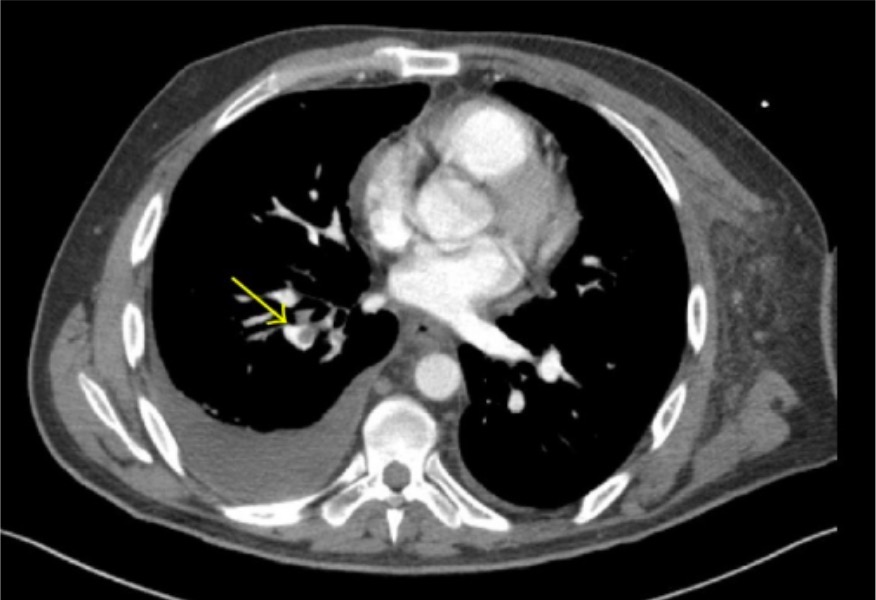
00:01 So, if you find that your patient has a pulmonary embolus, you’re gonna wanna go ahead and start treatment. 00:06 The treatment for PE is medication to help thin the blood. 00:09 Generally in the emergency department, we’ll go ahead and start heparin or a low-molecular weight heparin for all patients. 00:30 So, when you find your patient has a PE, you wanna go ahead and get this medication started as quickly as possible. 00:34 tPA is the other medication that should be considered to be given. 00:38 tPA is a more potent blood anticoagulant and we refer to it sometimes as a clot busting medication. 00:44 You wanna reserve this for patients who have cardiac compromise associated with their pulmonary embolus. 00:50 So, for patients who have a larger clot burden. 00:51 For patients who have a positive troponin. 00:55 Potentially for patients who have what we call a saddle embolus which is an embolus right at the bifurcation of the pulmonary vessels, almost looks like a saddle. 01:01 You wanna reserve this for patients who potentially have right heart strain on a bedside echocardiogram. 01:07 The other important point that I wanna make here is that if you think that your patient has a pulmonary embolus, you can actually give these medications prior to the official diagnosis being made. 01:19 So, if you have a very strong or a very high suspicion and your patient is critically ill or unstable, or potentially for a patient in cardiac arrest and whom you have a high suspicion, go ahead and get these medications onboard early. 01:31 For patients in cardiac arrest for a PEA arrest, this is one of the diagnosis that can potentially cause that, so you wanna go ahead and administer that tPA during that situation if you have a high suspicion. 01:43 So in conclusion for pulmonary embolus. 01:47 You wanna make sure that first and foremost, you’re thinking about this diagnosis. 01:50 Patients may present in a very subtle way. 01:54 When you’re thinking about it, go ahead and utilize your decision rules. 01:58 So, utilize the PERC rule and utilize Wells criteria to help you figure out your next steps. 02:02 But also, don’t undermine your clinical gestalt. 02:05 Your clinical gestalt can actually take you pretty far when you’re thinking about the pulmonary embolus diagnosis. 02:10 When you’re thinking about it, the next steps are either D-dimer testing for a low risk patient or further additional radiologic testing with either a CTA of the chest or a VQ scan. 02:23 Treatment for PE is heparin as well as tPA and you can get those medications on board early if your patient’s testing or evaluation and workup is delayed in any way.
About the Lecture
The lecture Pulmonary Embolism (PE): Management by Sharon Bord, MD is from the course Respiratory Emergencies.
Included Quiz Questions
In the management of pulmonary embolism, what is the recommended medication for patients with cardiac compromise or with a saddle embolus?
- tPA
- Heparin
- Aspirin
- Clopidogrel
- Warfarin
In the emergency department, what medication(s) may be given to a patient suspected to have pulmonary embolism but confirmation testing is delayed?
- Heparin or tPA
- High-dose aspirin
- Low-dose aspirin
- Clopidogrel
- Warfarin
Author of lecture Pulmonary Embolism (PE): Management

Sharon Bord, MD
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Great lecture given by a competent speaker. But Dr Bord let us down a little by not elaborating on a clinical teaching point and pearl of wisdom that she may have wanted to talk about in more detail. She makes several references to the subtle presentations PE can take and gives two personal examples in her introduction. She also encourages us to follow our gut instinct if PE is on our minds as a likely diagnosis. I have learnt that if you go looking for text book presentations then you are on the wrong track, and to some extent this lecture encourages us to think text book. One of the most confounding and frustrating aspects of PE is that it can present in many ways - it's a mischievous demon. For me shortness of breath is the only reliable symptom. I would like a warning given to include PE in the differential diagnosis of any patient presenting with shortness of breath. However, despite my warning PERC and Wells are a good aid for getting you out of a misdiagnosis, but you have to be thinking PE to begin with. If, as clinical educators, we pushed this point in 101 then perhaps more PEs could be picked up earlier.
