Playlist
Show Playlist
Hide Playlist
Acute Coronary Syndromes (ACS): Treatment and Assessment

-
Emergency Medicine Coronary Syndromes.pdf
-
Download Lecture Overview
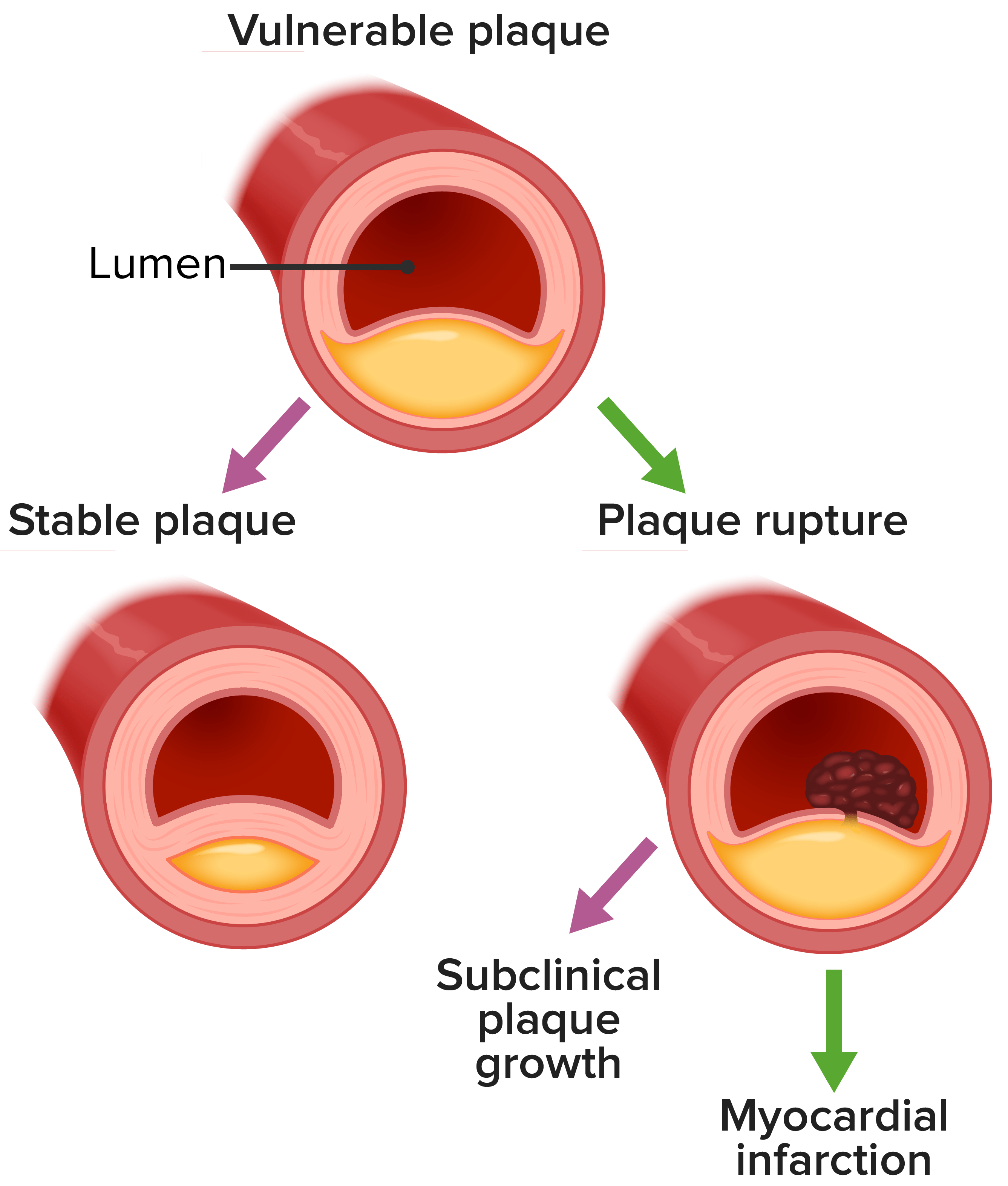
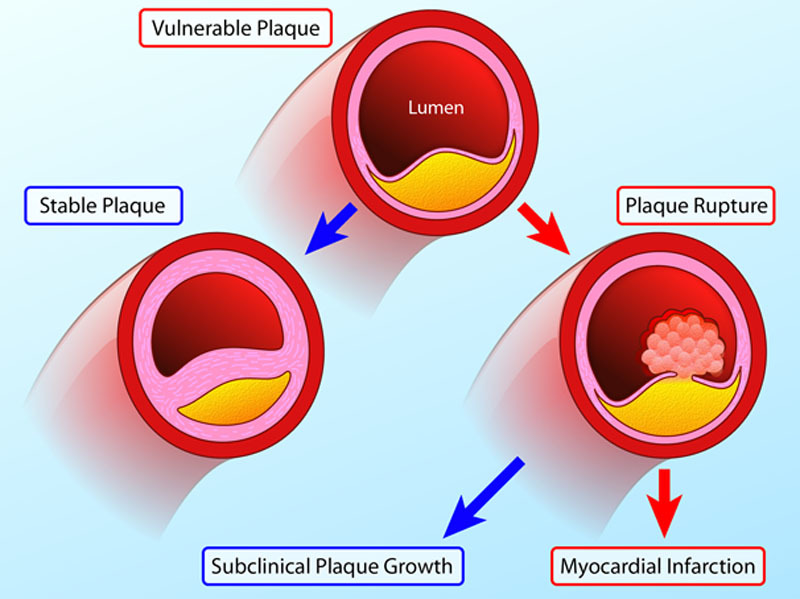
00:01 Hello. 00:02 Now we're going to talk about acute coronary syndromes a very common and important problem in the emergency department. 00:11 So coronary syndrome is actually very common. 00:13 In the United States, there are more than three quarters of a million cases of coronary syndromes each year. 00:20 The mean age is 68 years of age but the interquartile ratio goes from 56 to 79. 00:25 So this is really a disease process that affects pretty much all adults. 00:30 There is a male to female predominance. 00:32 So for every 10 patients with coronary syndromes six will be men for will be women. 00:40 And 70% of coronary syndromes are non-st segment elevations, meaning these are not acute MI's that are getting rushed to the cath lab. 00:49 These are patients who have more subtle findings or in some cases even no findings on their initial ECGs. 00:55 So recent trends when you look at the epidemiology of coronary syndromes shows that we're actually seeing fewer and fewer massive ST segment elevation events and more and more non-st segment elevation events. 01:10 So again, we're not seeing big acute coronary occlusions. 01:13 We're seeing more subtle ischemia. 01:16 Short-term mortality is stable across the board so there's not really been any change in the likelihood of people dying from coronary syndromes in the short term, but fortunately long-term survival is improving and that's largely due to improvements in diagnosis short-term and long-term management for these patients. 01:36 So what is a coronary syndrome? Very simply is an acute coronary syndrome is any new condition that leads to inadequate myocardial perfusion relative to demand. 01:49 So if the heart's not getting enough oxygen, it's not getting as much as it needs metabolically. 01:54 That is a coronary syndrome. 01:56 Now most coronary syndromes start with chest pain. 01:59 However, among patients with chest pain the vast majority are actually not having acute coronary syndromes although there is of course a significant overlap in the middle. 02:10 Among patients with coronary syndromes. 02:12 There's a continuum of disease. 02:14 So patients may have unstable angina patients may have non-st segment elevation myocardial infarctions or patients may have ST segment elevation myocardial infarctions. 02:27 So this is a continuum of disease acuity and there's different management depending on the patient's clinical presentation. 02:36 When we look at unstable angina. 02:39 We're generally talking about ischemic chest pain that occurs either while the patients at rest or with levels of exertion that they're normally able to tolerate I go out for a two mile walk every day Nd usually I'm fine abut in the past week, I'm getting chest tightness or getting short of breath within half a mile and I have to sit down that's an example of impaired exercise tolerance. 03:03 For these patients when they come see you in the emergency department. 03:06 They'll often have no ECG findings or their ECG findings will be very nonspecific and their lab abnormalities will be negligible as well. 03:15 So these patients are not going to typically present to you with elevated troponins. 03:19 By contrast, patients who have NSTEMIs or non-st elevation MI's these are patients who can have ischemic chest pain in any setting, it might only be with exertion. 03:30 It might be at rest. 03:33 When they present they will typically have some degree of EKG changes although a small percent will have none. 03:39 However, those changes are going to usually be st-segment depressions. 03:44 They're not going to be elevations because that's a different type of infarct and these patients are really characterized by their elevated troponin. 03:51 So they come in with chest pain. 03:53 They have EKGs that are not definitively diagnostic of an MI, but they show that they have elevated troponins. 04:00 And that's evidence of coronary infarction, that's our NSTEMI patient. 04:05 And then lastly we have our STEMI patients or patients with ST elevation MI size. 04:10 And these patients again, have chest pain that might occur at rest. 04:14 It might occur during exertion, but it's typically a single acute event and they're going to come in with the classic ST segment elevation that we all learned in medical school characterized acute myocardial infarctions. 04:29 Now for these patients, they will typically have elevated troponin, but we won't even see that in the emergency department because patients with STEMIs get emergent definitive treatment for their coronary disease and they're not going to be hanging around the ED for long enough for us to see there troponin is go up. 04:45 So that's going to be more of an inpatient finding and we're going to make that diagnosis based on EKG findings alone while they're in the emergency department. 04:56 So when we see patients with chest pain and we suspect coronary syndromes, we always want to get a rapid history and physical. 05:03 We want to know what was happening when the pain started. 05:06 How did it start? What did it feel like, what are all the circumstances surrounding this presentation? And we want to get an ECG and we want to do that very very quickly typically within 10 minutes of the time the patient arrives to the door. 05:20 If they're having a STEMI then they need to get a immediate definitive management. 05:26 So a STEMI tells you that the patient has complete occlusion of a coronary artery that is causing transmural full thickness infarct of part of their heart. 05:35 That's bad right, time is myocardium. 05:38 So these patients are going to go directly to cardiology and get definitive management, which we'll talk about in a minute. 05:45 If they're not having STEMIs, we have a little bit more time to think about them and we'll go through that algorithm second. 05:51 So here's a perfect example of a STEMI, you can see see in all the anterolateral leads. 05:57 So V2 V3 V4 V5 V6 also leads one and AVL you see tombstones, right? These are the classic convex ST segment elevation that we all learned about in medical school. 06:11 This is a STEMI. 06:14 So once again isoelectric baseline, which is highlighted in black, that's the PR segment and the TP segment, right? That's where the isoelectric base line is supposed to be. 06:25 If you look at the ST-Segment 1 millimeter after the QRS complex, which is by convention where we measure it, you can see with the new highlight that ST-segment is way up in the air above that Isoelectric base line. 06:40 So it's higher than it should be. 06:41 Isoelectric baseline, st-segment up above it, that's an ST segment elevation. 06:47 And again on this ECG, we're seeing it not just in the leads that are outlined but in several leads. 06:53 In order to diagnose somebody with a STEMI, I mentioned before we're using the ECG is our primary diagnostic tool. 07:00 So the patient of course has to have a history that's compatible with ischemic chest pain and they have to have ST segment elevation in two or more anatomically contiguous leads. 07:10 So in the anterior leads which are the two through V4, the lateral leads which are V5 and V6 and one in AVL or the inferior leads which are two three and AVF. 07:23 They have to have ST segment elevations two or more anatomically contiguous leads. 07:28 We're typically looking for two millimeters in men and 1.5 millimeters in women in especially V2 and V3 because that's a common place where you see non pathologic ST segment or J point elevation. 07:42 In all the other leads, we're looking for one millimeter of ST segment elevation. 07:47 So when you're measuring your ST segment, you want to make sure that you know 1. what your Anatomy is, so you want to know which leads go with which anatomical piece of the heart and again anterior is going to be V2 V3 V4. 08:01 Lateral is going to be V5 V6, 1 and AVL and inferior is going to be 2/3 and AVF. 08:10 So we want to know if they're anatomically contiguous and we want to know how high the ST segment is elevated relative to the standard for that particular lead. 08:21 The second criterion for ST segment elevation diagnosis is ST segment depression in V1 and V2, and very simply that represents posterior infarction. 08:32 And if you think about it, we always put ECG leads on the anterior part of the chest. 08:37 But if you're infarcting the back of your heart that image on your surface ECG is going to be inverted. 08:45 It's going to look upside down and backwards. 08:48 So ST-segment elevation zones that are occurring in the back of the heart will look like depressions when they're measured from the front of the body. 08:57 That's why V1 and V2 are special and ST segment depressions and those leads are considered to be ST-elevations for the posterior of the heart. 09:07 The final criterion is a new left bundle branch block, which of course this ECG does not demonstrate but if the patient has new development of QRS widening and a left bundle pattern that is also highly suggestive of a myocardial infarction. 09:21 So once the patient meets those criteria, what are we going to do about it? Well, first and foremost, we are very rapidly going to revascularize their coronary arteries. 09:32 So again ST-segment elevation means you've got complete occlusion of an artery that is causing transmural infarction of the heart that is not good. 09:42 We need to get that artery open back up and we need to save whatever myocardial tissue we can that's distal to it. 09:49 The best way to accomplish that by far is with percutaneous coronary intervention or PCI that refers to going to the cath lab performing angiography inserting stents to hold the coronaries open. 10:04 The other option that's available is thrombolysis that involves giving a clot-busting drug systemically. 10:10 However, it's not as effective as PCI and it's not as safe. 10:13 So any time you have the option of Performing PCI, that's always going to be the preferred technique provided you can do in a timely manner. 10:22 So the goal door-to-balloon time for PCI should be under 90 minutes. 10:27 If you're over 90 minutes, you don't think you're going to be able to get the patient to a center where they can perform PCI in a 90 minute timeframe. 10:36 Unfortunately that piece of heart that's distal to that included coronary artery is going to die. 10:42 So you need to go to plan B, which is going to be again systemic thrombolysis. 10:47 Now, we're using that less and less and less in modern times because there's more and more centers that are capable of Performing PCI. 10:55 But if you happen to be practicing in a limited resource setting thrombolysis might be your only option to save the threatened piece of the patient's myocardium. 11:05 So it is something we should be aware of in our armamentarium, even though we prefer PCI. 11:12 In addition to revascularisation while you're waiting for your patient to go to the cath lab you want to make sure that you optimize their medical management. 11:20 So we're going to give them antiplatelet therapy in the form of aspirin and an antiplatelet agent such as Clopidogrel or Ticagrelor. 11:28 We can also think about an oral beta blocker if there's no contraindication to doing that. 11:33 Now beta blockers in the acute setting are not nearly as important as they are long-term following the myocardial infarction. 11:40 But for patients who have significant hypertension or tachycardia on arrival, it might decrease strain on the heart and ultimately improve their outcome so you can think about it. 11:49 Although it's not mandatory to give up front. 11:53 We do definitely want to provide anticoagulation usually in the form of unfractionated Heparin for patients who are going to be going to the cath lab for the simple reason that in the event they have a bleeding complication. 12:05 We want to be able to turn it off and not have uncontrolled anticoagulants. 12:10 Kicking around round in their system preventing us from being able to control their bleeding. 12:16 And then lastly we want to think about analgesia. 12:18 So typically either nitroglycerin or morphine is used if there's not a contraindication. 12:23 Now morphine has been a little bit controversial lately because of some studies that have showed adverse outcomes associated with morphine, but it's still a reasonable thing to think about for a patient with chest pain that's refractory to nitroglycerine because we do want to alleviate our patients suffering in addition to giving them the definitive treatment that they need. 12:42 Recently fentanyl has replaced morphine in the management of acute coronary syndromes because fentanyl has a higher potency shorter onset and fewer side effects. 12:52 So that covers management for steady. 12:55 Now, let's go back to our ACS algorithm and consider the opposite possibility. 12:59 So we perform our history and physical, we're concerned about coronary disease. 13:03 We've performed our ECG looking for a STEMI, but now we haven't found one. 13:08 There is no criteria to send the patient to the cardiac catheterization lab. 13:12 So our next maneuver is going to be to assess their level of risk for coronary disease. 13:19 So for patients who don't have STEMIs, but you're still concerned about coronary syndromes. 13:25 We want to assess their level of risk for coronary disease. 13:28 This is our first priority in patients in whom we suspect a coronary syndrome who were not sending to the cath lab. 13:35 There are a number of different decision tools out there to help us do that. 13:38 But the one we use most commonly in the ED that's been validated for use in our setting is called the heart score. 13:44 It consists of five elements which conveniently spell the word heart. 13:48 So the first element is history if your patient has a very concerning history, they get 2 points, if they have a so-so history, they get 1, and then if the history is minimally suspicious they get 0. 14:00 For ECG changes, it's based on ST segment depressions. 14:05 ST depressions are pretty characteristic of coronary ischemia, and there aren't a lot of other conditions that cause those so you get 2 points for those. 14:13 Whereas if you have nonspecific changes or no changes, you get fewer points. 14:18 Age is the next variable aged over 65 gets you 2 points, 45 to 65 gets you 1. 14:25 And if you're under 45, you're much less likely to have a coronary syndrome. 14:29 So you get no points for that. 14:32 Risk factors address the classic elements of risk for coronary disease and we'll talk about those in just a few minutes. 14:39 If you have one or two risk factors you get 1 point. 14:42 Greater than three. You get 2 points. 14:44 No risk factors. Obviously you get none. 14:47 The last variable is our troponin. 14:49 So if your troponin is more than three times the upper limit of normal for your institution that gets you 2 points. 14:56 If you have a small troponin leak just a little bit of an elevation that's less than three times that upper limit of normal you get 1 point, and normal troponin is get you no points. 15:06 Now like I said, this is not the only tool that's out there but it is a very useful tool that has been validated in the emergency department to predict MACE or Major Adverse Cardiac Events and that's really our goal. 15:21 We want to identify the patients who are at high risk of having another MI of having an adverse outcome like death so that we can address their needs urgently and we want to identify low-risk patients so we can send them home and not perform a lot of unnecessary tests on them. 15:39 So that's the purpose of this type of a scoring system.
About the Lecture
The lecture Acute Coronary Syndromes (ACS): Treatment and Assessment by Julianna Jung, MD, FACEP is from the course Cardiovascular Emergencies and Shock. It contains the following chapters:
- Introduction
- STEMI
Included Quiz Questions
Which of the following statements regarding acute coronary syndromes (ACS) is FALSE?
- ACS includes STEMI, NSTEMI and stable angina
- It is common in the United States.
- It most commonly affects adults.
- It is more common in men.
- About 70% of cases do not show ST-segment elevations.
Which one of the following statements best describes unstable angina?
- Ischemic chest pain occurring with previously tolerated levels of exertion
- Elevated troponin levels occurring in association with chest pain
- ST-segment elevations when chest pain is present
- Ischemic chest pain in any setting
- Elevation of CK-MB levels occurring in association with chest pain
What anatomic region of the heart is represented by leads II, III, and aVF?
- Inferior
- Anterior
- Left lateral
- Right lateral
- Posterior
Which of the following statements is incorrect regarding ST-elevations in STEMI?
- ST-elevations should be observed at least in one lead.
- ST-elevations should be more than 2 mm in men in V2-V3 leads.
- ST-elevations should be more than 1.5 mm in women in V2-V3 leads.
- Elevations must be at least 1 mm in limb and most precordial leads.
- Non-pathologic ST elevations are common in V2-V3 leads.
What is the ‘door to balloon’ goal time for PCI?
- Less than 90 minutes
- 140 - 160 minutes
- 120 - 140 minutes
- 100 - 120 minutes
- 90 - 100 minutes
Which of the following is not evaluated in the HEART score for chest pain patients?
- Tachycardia
- History
- ECG
- Age
- Risk Factors
Author of lecture Acute Coronary Syndromes (ACS): Treatment and Assessment

Julianna Jung, MD, FACEP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I just love how you explained everything in 5 min so clearly when I browsed for so long. Very useful information
Very useful information delivered in a direct and easy to understand manner.
