Playlist
Show Playlist
Hide Playlist
Hirsutism: Differential Diagnosis, Examination and Management


-
Slides Hirsutism ReproductiveEndocrinology.pdf
-
Download Lecture Overview
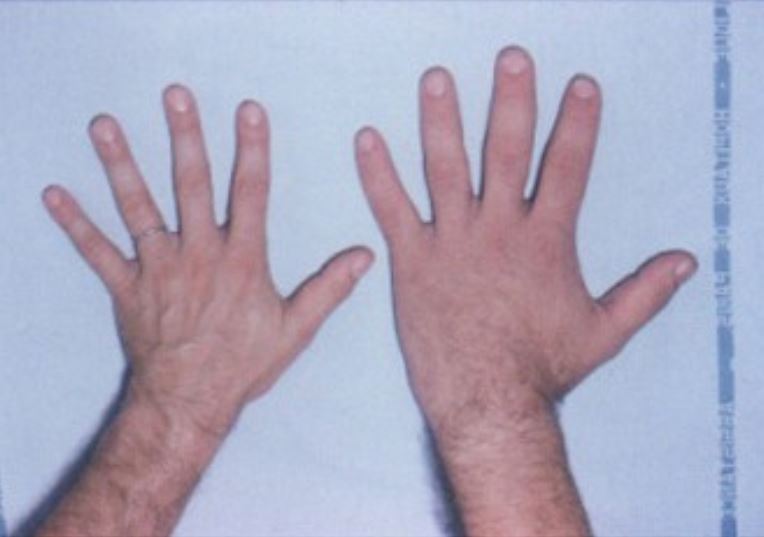
00:01 Let’s now review the differential diagnosis of hirsutism. 00:04 There can be non-androgenic causes of hirsutism, one of those being acromegaly. 00:10 Here I have a picture of a patient in her younger years versus her later years. 00:15 Is there anything you notice about the patient besides her aging? Have you guessed it? I’ll give you a hint, look closely at her features. 00:33 Well, if you said her features look coarse, then you’re correct. 00:42 This is very common with acromegaly and this is a cause of hirsutism. 00:49 You can also have hirsutism with skin irritation such as with the application of Retinoic Acid. 00:55 Certain medications can also lead to hirsutism including cyclosporine, phenytoin, minoxidil, calcium channel blockers, and also other medications listed here. There are again androgenic causes. 01:10 We have a whole lecture set entitled PCOS where you can learn more. 01:14 There is another phenomenon called the HAIR-AN syndrome and for more information, download the slides associated with this lecture. 01:22 There’s also something called idiopathic hirsutism. 01:26 We really don’t know why but we think it’s intimatic activity at the level of the hair follicle. 01:32 Then there’s non-classical CAH, for more information about congenital adrenal hyperplasia, please see the slides entitled CAH or congenital adrenal hyperplasia. 01:43 And then very rarely, we can see androgen-secreting neoplasms in the ovary or the adrenal. 01:49 Recall that elevated prolactin can also cause hirsutism. 01:54 Luteoma of pregnancy can also be an androgenic cause and this usually happens when the placenta also has some issue as well. 02:04 Theca-Lutein cycsts are also associated with high maternal serum hCG. 02:09 Remember that Cushing syndrome is a differential diagnosis in hirsutism. 02:14 This is often tested during the USMLE so pay close attention to the next slides. 02:20 Are you ready? Here we go. Let’s rule out Cushing syndrome. 02:25 What are the signs of elevated cortisol in a patient who presents with hirsutism? They may have fat accumulation around the face and neck. 02:36 They may have a buffalo hump but this can also be seen in just an obese patient. 02:41 They typically have central obesity, that means obesity around the abdomen and belly, one distinguishing feature though is purple striae, these are not normal stretch marks as you can see in panel B, this patient has purple striae. 02:57 They appear purple as opposed to dark like normal stretch marks. 03:02 This is because you can see the vessels in the thin skin of a patient who has elevated cortisol. 03:07 If you see this in a patient, you definitely need to obtain a 24-hour urinary cortisol. 03:14 You may need to do this on several occasions before you can make a diagnosis. 03:19 There are other tests regarding elevated cortisol that you can find in other lectures. 03:24 Upon physical exam, you can find hair growth in a male distribution pattern. 03:30 Traditionally, we use a Ferriman-Gallwey score, and a score greater than 8 was associated with hirsutism. 03:37 However, 25% of patients who have hirsutism use some sort of cosmetic treatment for excessive hair including bleaching, plucking, shaving, and threading. 03:48 So this has become less useful as a clinical assessment but it’s important to know. 03:53 Let’s now go over a checklist. If you see evidence of cliteromegaly, you should think that this patient has androgen excess. 04:02 What if she has galactorrhea, what would you expect? If you said elevated prolactin, that’s correct. 04:10 Sometimes you can see abdominal or pelvic masses that can actually secrete androgens which lead to hirsutism. 04:18 Treatment of hirsutism is aimed at reducing the production or increasing the binding, and/or blocking the action of androgens. 04:27 Since PCOS is by far the most common cause of hirsutism, oral contraceptive pills are the first line therapy. 04:35 The management of PCOS is discussed in a later lecture but let’s review it here. 04:43 Sixty to 100% of women who report hirsutism and then use OCP’s, have subsequent improvement. If other medications are used, a woman must be on contraception to prevent any anti-androgen effects on a male fetus. 04:57 Oral contraceptive pills decrease LH secretion from the anterior pituitary. 05:03 This results in less LH stimulation of the theca cells in the ovary which ultimately leads to decreased testosterone production. 05:12 If there’s decreased testosterone, you guessed it. There’s less free testosterone. 05:17 Also, the estrogen in the pill increases sex hormone binding globulin which binds more free testosterone. 05:25 Remember in addition to actually suppressing LH secretion, estrogen stimulates sex hormone-binding globulin production. 05:39 Also, oral contraceptive pills decrease adrenal production of DHEA-S and we think that progestins in contraceptives actually inhibit 5-alpha-reductase activity in the skin. 05:51 There are other medications that we can use instead of oral contraceptive pills or with oral contraceptive pills. These include medications that actually block androgen action. 06:03 One of these is spironolactone, it’s an aldosterone antagonist and a mild diuretic. 06:09 It’s an effective therapy because it actually blocks the androgen receptor, decreases 5-alpha-reductase, and competes for the binding of testosterone with sex hormone-binding globulin. Flutamide is another alternative. 06:22 However, caution, this may be on your USMLE exam, there have been reports of liver enzyme abnormalities and hepatitis. 06:30 Also, these patients get green urine which can be very distressing and excessive dryness of skin and scalp hair. 06:38 However, it is known to be an androgen receptor blocker and it’s as effective as spironolactone. In the US, we do not have access to CPA, however in other countries they do. 06:51 This is a strong progestin and it’s an antiandrogen that decreases circulating testosterone and androstenedione. Finally, there’s finasteride which is a 5-alpha-reductase inhibitor. 07:03 There are also some cosmetic solutions for hirsutism. 07:08 Remember that even if you treat hirsutism with an OCP or other medical management, the effect will not be immediate. 07:16 So patients still need to participate in cosmetic removal of hair. 07:20 This can include laser hair removal, electrolysis, topical creams, and this cream is actually a cream that actually inhibits the enzyme active in the dermal papillae that’s essential for hair growth. 07:35 However, it is very expensive and it’s usually not covered by insurance in the US. 07:39 Women can also undergo waxing, normal shaving, threading, and different agents that will actually cause the hair to fall out. 07:48 Thank you for listening and good luck on your exam.
About the Lecture
The lecture Hirsutism: Differential Diagnosis, Examination and Management by Lynae Brayboy, MD is from the course Reproductive Endocrinology. It contains the following chapters:
- Differential Diagnosis of Hirsutism
- Physical Exam; Medical Management
Included Quiz Questions
Which of the following is a non-androgenic cause of hirsutism?
- Acromegaly
- PCOS
- Idiopathic hirsutism
- Non-classical CAH
- Arrhenoblastoma
Which of the following medications does NOT result in hirsutism?
- Thiazides
- Minoxidil
- Erythropoietin
- Cyclosporine
- Calcium channel blockers
A 22-year-old woman patient presents with excess fat accumulation on the back, purple striae, and increased facial hair. Which of the following laboratory tests is needed to confirm the suspected diagnosis?
- 24-hour urinary cortisol
- Urine cortisol levels
- Serum cortisol
- Dip stick testing
- RBC cortisol levels
What score is considered hirsutism, according to the Ferriman-Gallwey method of assessment?
- 8 and above
- 6 and above
- 4 and above
- 2 and above
- 1 and above
Which of the following is the most common cause of hirsutism?
- PCOS
- Hyperprolactinemia
- Theca lutein cysts
- Pregnancy luteoma
- HAIR-AN syndrome
A 25-year-old obese woman comes with jaundice and laboratory studies show elevated liver enzymes. She has a history of PCOS and is undergoing treatment. Which of the following drugs for the treatment of PCOS could have caused this presentation?
- Flutamide
- Spironolactone
- Cyproterone acetate
- Finasteride
- Eflorithine hydrocholride
Author of lecture Hirsutism: Differential Diagnosis, Examination and Management

Lynae Brayboy, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Concise and covered the needed material. Along with providing the differential diagnosis to pay attention to.
