Playlist
Show Playlist
Hide Playlist
Community-acquired Pneumonia (CAP): Pathology, Diagnosis, Signs & Symptoms

-
Slides Pneumonia Alverson.pdf
-
Download Lecture Overview
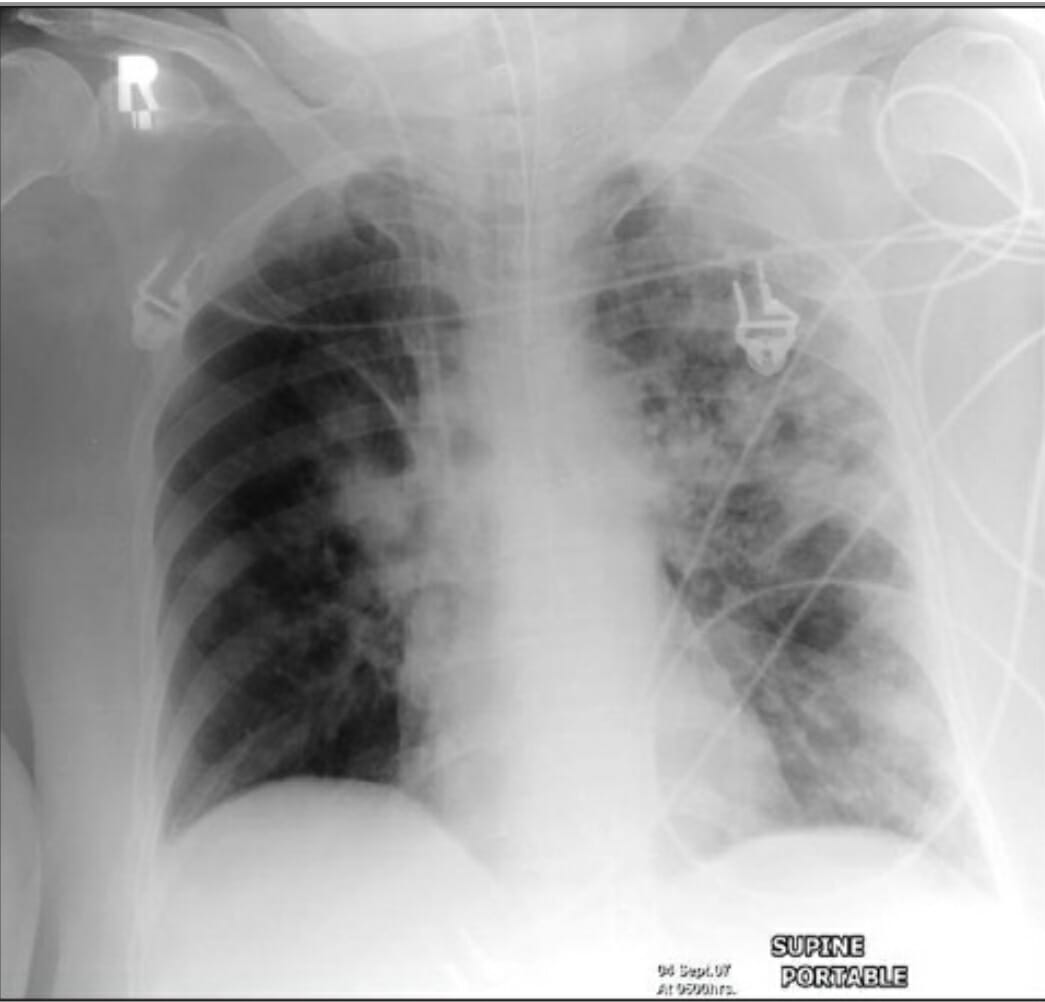
00:00 In this lecture we're going to discuss Pediatric Pneumonia. Pediatric pneumonia is an infection of the lower airways of children. It typically presents with respiratory distress, hypoxemia, cough and fever. In the entire world, it's actually the 3rd leading cause of death of children and it's a common cause in the United States of hospitalization. Most community acquired pneumonia is viral. It's not usually caused by a bacteria but distinguishing between viral and bacterial disease is almost impossible. 98% of blood cultures in children who we suspect of having bacterial disease are in fact negative and a quarter of infants who are healthy will test positive for a virus by nasal PCR which means that if we use a viral nasal PCR as a test, we're going to get a lot of false positives. So what are the organisms that are most likely to cause pneumonia in children? Well, under 3 months of age, it's still likely <i>Strep pneumo</i> but in those children who are just a few weeks of age it could be <i>Chlamydia trachomatis</i> from the mother. Also from the mother it could be group B strep or <i>E. coli</i> or less common but it can absolutely happen in <i>Staph</i> <i>aureus</i> pneumonia. In infants and children, the organisms are a little bit different. Still, among the bacteria, <i>Strep pneumo</i> is the most common followed maybe by <i>H. flu</i> and <i>Staph aureus</i> and <i>Mycoplasma pneumonia</i> can happen in kids over 5, is a little bit less common in kids under 5. 01:43 However, there are exceptions to that rule. There are a couple special circumstances we have to keep track of though. Children who've traveled and have a long malingering disease might have tuberculosis. Children with cystic fibrosis might have Pseudomonas species. Children who've been exposed to Legionella could have that and also fungal diseases are popular especially in children with T-cell deficiency. Also, we're not sure but perhaps <i>Chlamydia</i> <i>psittacosis</i>, <i>Coxiella</i>, various parasites, these can very rarely arise under very special circumstances but generally the bug we're most concerned about in terms of bacteria across the board is <i>Strep pneumoniae</i>. 02:28 Let's look at how children present based on their age. Neonates are more likely to present with non-specific symptoms like fever, lethargy, or just apnea compared to infants who often have tachypnea, fever, cough and very commonly abdominal pain. These children tend to have minimal upper respiratory infections. So, minimal upper respiratory infections in the setting of pulmonary disease is more concerning for a bacterial illness as opposed to a viral illness. If a child has a lot of runny nose, it's more likely to be a virus. So, what do we see on exam that's specific to community acquired pneumonia? Well, the first and most important thing is rales. Rales which is also sometimes called crackles is that high-pitched sound we hear on inhalation and exhalation in a focal point over some infected lung. Patients on percussion may have dullness to percussion. 03:29 Patients may have areas where there's decreased aeration. You can't hear those breath sounds so well and wheezes are more common in viral disease than they are in true lobar bacterial pneumonias. A chest x-ray in a well-appearing infant increases the risk of unnecessary antibiotics and does not necessarily distinguish between bacterial and the vastly predominant viral disease. 04:01 What I'm saying is if you believe an infant who's relatively well-appearing has pneumonia based on your exam, you should not get a chest x-ray, just treat the pneumonia. If that child has a question of pneumonia but you have a reassuring exam, getting a chest x-ray increases antibiotic use without benefit. In other words, probably safe to assume they do in fact have a viral illness. 04:29 The white count on a CBC in no way distinguishes between viral and bacterial disease. It does not help at all. So there's really no rule for a white count in distinguishing between viral and bacterial disease. Viral swabbing in the nose has a high false positive rate. So it's unclear that a child couldn't have a bacterial illness even if they have a positive nose swab. So that test is somewhat useless as well. So what is useful? Well, if a child is being hospitalized, it is important to get a chest x-ray. That's because there is an increase rate of complicated pneumonia or pneumonia with effusion that's going on and the chest x-ray can help you decide if you need to get in fact a chest tube in addition to your antibiotics. So it distinguishes between complicated pneumonia and uncomplicated pneumonia. It also distinguishes between bronchopneumonia and lobar pneumonia. A lobar pneumonia is very much likely to be a bacterial pathogen whereas scattered patchy disease that's diffuse is more likely to be viral. Occasionally, the x-ray will pick up this complicated pneumonia we talked about. This is where pus has accumulated in the wall between the chest wall and the lung in the pleural space. In this x-ray right here, you can see that this pleural space is remarkably filled with a large amount of pus and it's going all the way up to the side of the chest wall. That's something you want to look out for because this patient here is probably going to be treated differently than a patient who doesn't have this.
About the Lecture
The lecture Community-acquired Pneumonia (CAP): Pathology, Diagnosis, Signs & Symptoms by Brian Alverson, MD is from the course Pediatric Infectious Diseases. It contains the following chapters:
- Pathology of Community Acquired Pneumonia
- Signs and Symptoms of Community Acquired Pneumonia
- Diagnosis of Community Acquired Pneumonia
Included Quiz Questions
What does a WBC count of 25,000/mm3 on a CBC in a child with pneumonia indicate?
- An infectious etiology
- A bacterial infection
- A fungal infection
- A viral infection
- Foreign body aspiration
Which of the following is NOT a common cause of pneumonia in a patient who is less than 3 months of age?
- Moraxella catarrhalis
- Streptococcus pneumonia
- Chlamydia trachomatis
- Group B streptococcus
- E. coli
Which of the following tests are useful in differentiating a viral versus a bacterial cause of pneumonia in children?
- None of the options
- Chest X ray
- WBC count
- Complete blood count
- Swabbing of the nose
What is the purpose of performing a chest X-ray in a hospitalized patient with pneumonia?
- It helps identify complicated pneumonia.
- It helps differentiate bacterial versus viral pneumonia.
- It helps the choice of treatment.
- It helps in providing definitive diagnosis of organism.
- It can diagnose a rib fracture caused by coughing.
Which of the following organisms typically causes pneumonia in a child with cystic fibrosis?
- Pseudomonas
- Chlamydia
- Tuberculosis
- Legionella
- Coxiella
Author of lecture Community-acquired Pneumonia (CAP): Pathology, Diagnosis, Signs & Symptoms

Brian Alverson, MD
Customer reviews
4,5 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
2 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent lecture. One of the best lecture, along those on Asthma and bronchiolitis. Tons of pearls and clear explanations for decision-making for the practicing clinicians.
I would like subtitles in spanish in the lecture. The automated subtitles are mistranslated. However Dr. Brian Alverson is very clear in his explanations !
Me gustaría que hubiera subtítulos en español en cada vídeo. o contrataran traductores
Really helpful, very clear both for didactic & clinical parts. Thanks!
