Playlist
Show Playlist
Hide Playlist
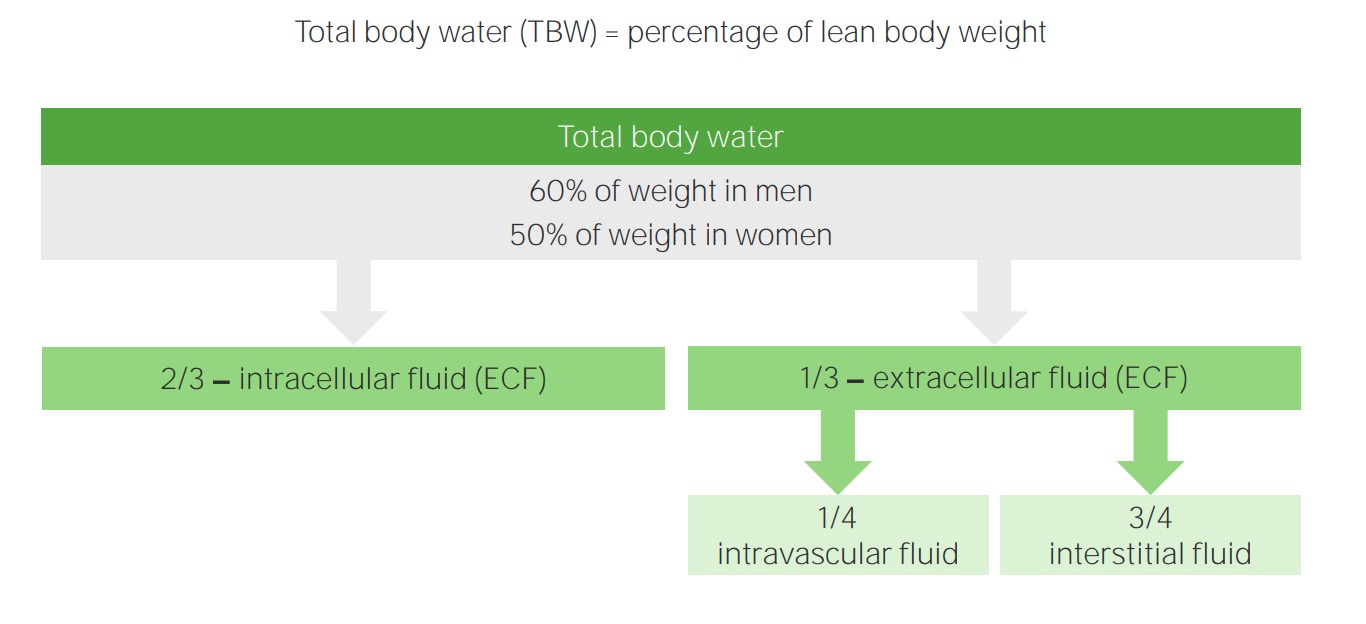
Extracellular Fluid (ECF) and Intracellular Fluid (ICF): Changes in ECF Volume

-
Slides WaterandSodiumPathophysiology RenalPathology.pdf
-
Download Lecture Overview
00:01 Now, what this basically means with ECF volume is the following. What if we have too much or too little, what kind of signs meaning you the clinician, are going to find in your patient? If that patient has lost too much sweat, what does the skin do? You decrease skin turgor, what does that mean? Well right now, you won't be able to see that in me because I am pretty well hydrated, in fact I am kind of a camel. I keep drinking and drinking and drinking and I will never, well as far as the lecture series are concerned, you will not find decreased skin turgor in me. However, say that I wasn't drinking water and I am going 8 to 10 hours of just lecturing. That is a lot of perspiration is taking place through evaporation. And maybe perhaps I am feeling a little dehydrated, but anyhow point being is I am being dramatic here. What if your patient has lost quite a bit of sweat and their blood pressure has decreased and then their skin is able to then tent. You pull it up and then it remains as such. That is called decreased skin turgor, why? Because here literally you have lost the plasma compartment. So, therefore, the ECF has diminished in terms of its size or its contraction process versus if you had hypervolemia. If there is hypervolemia obviously, you wouldn't have decreased skin turgor. 01:31 That becomes important in terms of being too little. Decreased skin turgor equates to skin tenting. Look for that description, understand as to what we're describing. On the opposite end of the spectrum, if you had too much ECF, though not only might you have too much in the plasma, but at some point maybe it is leaking out into the interstitium. Give me examples. 01:57 Congestive heart failure, would mean what? What do I mean by that? What am I asking you? Well, what is it that is causing increased fluid in the ECF in congestive heart failure when you have decreased cardiac output? It is the increase in which Starling's force? Hydrostatic pressure. Good. You are pushing the fluid into the interstitium. Is that too much or too little in the ECF? That is too much. 02:28 We will talk about the feedback mechanism further where you should know that in congestive heart failure because the fluid is escaping the vasculature or in other words the plasma compartment is going into the interstitium. Guess what is going on the kidneys. Decreased perfusion and you are releasing renin and this viscous cycle of RAAS especially the aldosterone and pushing that fluid into the interstitium. We will continue unless you crack the underlying issue of a dysfunctional heart. What is my topic? Too much. But you see as to how much detail we have just gone into so that you get the full clinical picture. You are not just memorizing this. What if there was a protuberance stomach in a patient maybe perhaps I am giving you a couple of stereotypical situations and that is what medicine is, isn't it? Where is your patient coming from? Developing country, developed country. What kind of exposure has your patient had? Did they live in an apartment where maybe there was fire mean to say gas is escaping? All of this becomes very relevant, why? Because everything that we are doing ladies and gentleman, most common presentations. If you find a patient, you might be from a developing country where just perhaps, the child may not have had access to food properly, malnutrition specifically protein. Are you with me? So if there're lack of proper protein consumption in this child. Wow! What is this called? Kwashiorkor. Why did I emphasize the -orkor? Kwashiorkor is lack of proper protein consumption whereas if it is marasmus, it is total caloric malnutrition. Let us go back to Kwashiorkor. If your child is not consuming proper amounts of protein, then what then happens? You lose the oncotic pressure. 04:23 Are you with me? So now you have lost oncotic pressure, so you are not able to properly do what? Maintain and contain your fluid in the vasculature. Now for a different reason, we have now lost fluid from the plasma compartment and has now gone into the interstitium. Interesting. 04:43 So this is Kwashiorkor or let us say that there is Northan Africa where in Egypt, in microbiology, you have learned that there is a common organism that then cause damage to the liver. Schistosomiasis you have heard of before. That schistosomal organism has a propensity of affecting and injuring the liver to the point where the liver gets damaged. 05:06 What happens? You cannot produce proper amounts of what? Albumin. Same concept. What happens? Decreased oncotic pressure and your patient may have a protuberance stomach. What is this? This is ascites. Do you get my points now? We talked about too little with decreased skin turgor because of loss of fluid or there might be accumulation of too much fluid in the ECF and I have given you congestive heart failure and I have also given you an example such as liver damage or maybe perhaps Kwashiorkor. Let us continue. Everything that you do in physiology, any subject as you can see here immediately give it a clincial tag, you cannot go wrong and this information will stick.
About the Lecture
The lecture Extracellular Fluid (ECF) and Intracellular Fluid (ICF): Changes in ECF Volume by Carlo Raj, MD is from the course Fluid and Electrolyte Balance.
Included Quiz Questions
What causes skin tenting in the setting of low blood pressure?
- Decreased effective circulating volume
- Decreased oncotic pressure in the plasma compartment
- Ineffective circulation of blood due to heart dysfunction
- Loss of isotonic fluid
- Increased hydrostatic pressure in the plasma compartment
What is the etiology of marasmus?
- Lack of total caloric nutrition
- Lack of protein nutrition
- Too much fluid in the extracellular compartment
- Urinary albumin loss
- Inability to form albumin
What type of pressure is responsible for the development of edema in congestive heart failure?
- Increased hydrostatic pressure in the plasma compartment
- Increased oncotic pressure in the interstitium
- Increased hydrostatic pressure in the interstitium
- Decreased hydrostatic pressure in the plasma compartment
- Decreased oncotic pressure in the plasma compartment
What is responsible for the development of ascites in a patient with schistosomiasis?
- Inability to produce albumin
- Dysfunctional liver metabolism
- Excessive hydrostatic pressure
- Protein wasting in the urine
- Insufficient protein intake
Author of lecture Extracellular Fluid (ECF) and Intracellular Fluid (ICF): Changes in ECF Volume

Carlo Raj, MD
Customer reviews
2,7 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
2 |
| 1 Star |
|
0 |
man i really find it hard to understand the lectures
I LOVE the lecture but i'm having difficult time understanding it. I had to watch and stop and write to understand it.. maybe more diagrams? or break it down :)
not really engaging, hard to hear and understand. Didn't understand some of what he was saying
