Playlist
Show Playlist
Hide Playlist
Hyperkalemic Cardiac Arrest – Drug Induced Emergencies

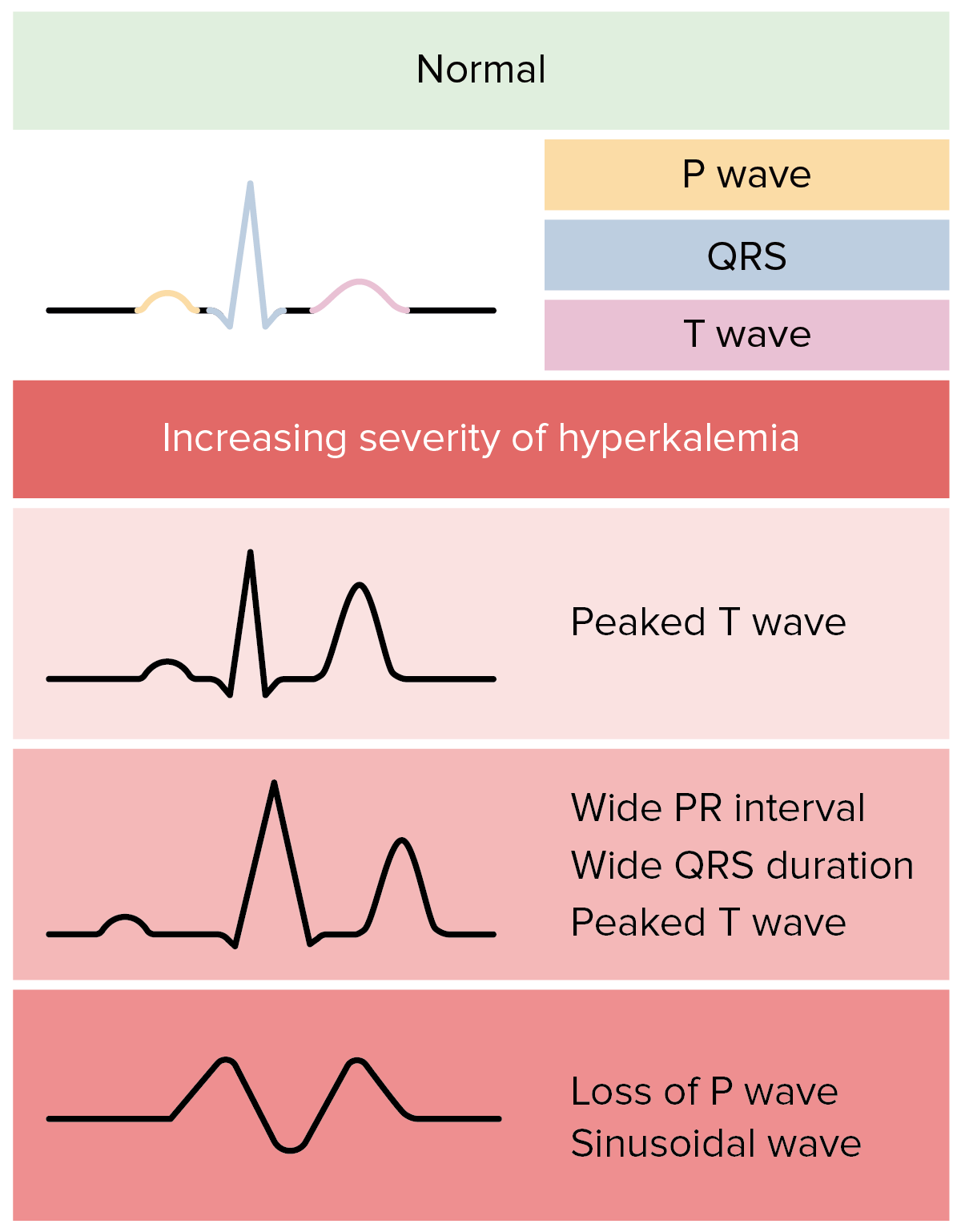

00:00 So, Hyperkalemic Cardiac Arrest. Hyperkalemia is high potassium in the bloodstream. Normally, potassium is very narrowly controlled in our blood stream. A lot of potassium inside our cells, but not a lot in the bloodstream itself. And the kidneys are responsible for excreting potassium and our gut is responsible for absorbing potassium. And our bodies homeostatic mechanisms are in place to control the level of potassium. But if potassium is given by the physician or through some error by a nurse in the ICU, or if you give Succinylcholine to the wrong patient, you can have a very sudden increase in potassium. 00:45 So normally a potassium, we'll say, runs around 4 mEq/L. 00:51 If you give that patient, normal patient, Succinylcholine, their potassium will go up to about 5 mEq/L, which is not a problem. If however you start at a higher level, for instance in a patient with a renal failure who hasn't been recently dialyzed, let's say it starts at 6, and you give them Succinylcholine, it may go up to 7 or 8 and there'll be a cardiac arrest. 01:15 In addition, if you give Succinylcholine to people who have conditions such as neurologic problems, massive trauma, spinal cord injuries, recent burns, burn in the last year actually, or renal failure, there can be a huge release of potassium into the bloodstream. And what happens with the ECG, and it happens over a minute or two, is the t-waves, which is the last wave in the normal complex of the ECG suddenly become peaked, and then the whole complex starts to widen. And then you can get what's called a sine-wave where the, it looks kind of like this, it looks like waves on the sea. And then asystole. An asystole is complete loss of contraction of the heart, complete loss of electrical activity in the heart. What happens with Hyperkalemia is, there's a change in the ratio between the resting potential and the threshold potential in the sino-atrial node, which controls our heart rate. This is a complex concept and I'm not going to spend a lot of time on it because it really requires you to sit down and read in detail if you're interested. But what happens is that, by changing the ratio of resting potential to threshold potential, the heart is unable to produce electrical signal that will cause an action potential and cause a wave through the heart. 02:51 The only treatment for this that works quickly is to either lower the potassium, and unfortunately it's hard to do that quickly, or to give a drug that interacts with potassium to change that ratio of threshold to resting potential back towards normal. And the drug that you gave is Calcium. Calcium is never given in normal cardiac arrest situations, because in ischemic cardiac arrest it can actually cause cell death and it no longer exists on the ACLS protocol. So this is an asystolic cardiac arrest where you don't use the ACLS protocol, you use calcium. 03:33 This will very rapidly change that ratio and amazingly, the normal heart rhythm will come back again. It doesn't however have any effect on the elevated potassium level in the blood. And you must treat that. And there are a number of ways of treating that, including hemodialysis in which you actually take the potassium right off. You can give glucose or insulin intravenously and that drives potassium back into the cells. Or, if you've got a patient where it's not a huge problem, it's not that badly elevated and you just want to bring it down over a couple of days, you can use an exchange resin such as Kayexalate orally. 04:15 And that'll help clear the potassium out of the system. 04:21 So hyperkalemic cardiac arrest is, as I mentioned, it's an uncommon event, but I've seen it several times. It does not follow the ACLS guideline, so you have to be aware of that. The treatment of the Hyperkalemia is necessary even if the patients return to a normal heart rhythm. So you can't forget that! And I've seen one death because the physician involved sent a patient to the ward assuming that, because the rhythm was back to normal, all was well. And the patient had a recurrence of the hyperkalemic cardiac arrest on the ward and unfortunately didn't survive.
About the Lecture
The lecture Hyperkalemic Cardiac Arrest – Drug Induced Emergencies by Brian Warriner, MD, FRCPC is from the course Emergencies.
Included Quiz Questions
In which of the following patients can succinylcholine be safely administered?
- A 23 year old male with Type I Diabetes Mellitus
- A 13 year old male with extensive burns suffered in the last month
- A 45 year old woman who has missed her last week of dialysis
- A 35 year old male with T5 spinal cord injury causing paraplegia
- An 18 year old female who suffered massive trauma two weeks ago
What is the initial ECG sign seen in impending hyperkalemic cardiac arrest?
- Peaked T waves
- Asystole
- Sine Wave
- Prolonged QT complex
- Rsr' in lead aVR
Author of lecture Hyperkalemic Cardiac Arrest – Drug Induced Emergencies

Brian Warriner, MD, FRCPC
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Thank you for highlighting the important aspects to remember during a Hyperkalemic Cardiac arrest.
