Playlist
Show Playlist
Hide Playlist
Trauma: Circulation, Disability & Exposure



-
Emergency Medicine Trauma.pdf
-
Download Lecture Overview
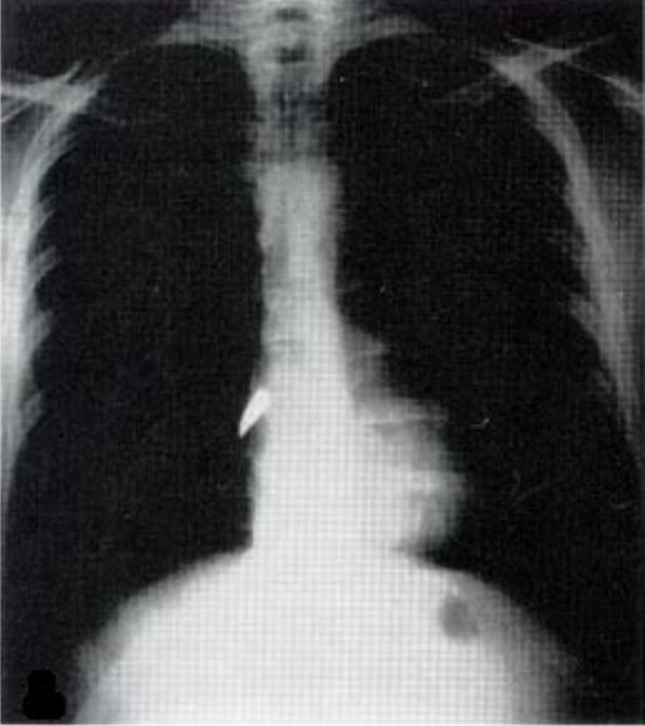
00:01 Moving on to C. 00:03 Circulatory insufficiency is very common in trauma. 00:06 Obviously, trauma is associated with bleeding. 00:09 So we very often see patients who have significant blood loss and circulatory compromise as a result of that. 00:16 The things you wanna look for when you're thinking about a patient circulation is just their overall appearance. 00:22 Are they pink and perky? or are they pale, or cyanotic, or altered? These are things that should help you get sort of an overall global sense of the adequacy of their perfusion. 00:33 You can also look at things like capillary refill, and obviously, you wanna look for signs of external bleeding, because a patient who has a wound that’s actively hemorrhaging, you're clearly gonna wanna control that bleeding before you do much of anything else. 00:46 We also wanna feel their peripheral pulses. 00:49 And the peripheral pulses are really important because they give you a quick sense of the patient's blood pressure, which is really the bottom line on the adequacy of their perfusion. 01:00 So a patient who has a nice, bounding, easily palpable dorsalis pedis pulse, has a systolic blood pressure of 90 or more. 01:09 So that’s a pretty quick way if you feel those dorsalis pedis pulses and you're satisfied that they’re palpable and normal, that is a pretty quick way to say, "Yeah. 01:18 “You know what? My patient's circulatory status is probably adequate at least right at this moment.” Moving farther proximally, radio pulses indicate a systolic of at least 80. 01:29 Femorals can indicate a systolic of at least 70. 01:33 And you don't lose your carotid pulse until your systolic goes below 60. 01:38 So really, getting a feel for which pulses are present, and which pulses are absent, can give you a pretty accurate sense of what your patient's blood pressure is and whether or not their perfusion is adequate. 01:49 Of course, once you get your patient hooked up to the monitor, you wanna know what their heart rate is, and you wanna know what their blood pressure is because these are our circulatory vital signs and they're gonna be used to guide our resuscitation and help us decide whether or not our resuscitative efforts are effective. 02:07 So our big circulatory life threat, like I already mentioned, is gonna be hemorrhagic shock. 02:13 Trauma is strongly associated with blood loss and this is by far the most common cause of death among traumatically injured patients. 02:21 However, we wanna consider other causes of shock as well, specifically tension pneumothorax and cardiac tamponade. 02:28 Both of these are forms of obstructive shock, where the injury prevents normal blood flow back to the heart from the venous circulation and impairs cardiac output that way. 02:40 Again, we're gonna talk about both of these disease entities in some detail in future lectures, but you should be aware that not all shock and trauma is gonna be related to hemorrhage. 02:51 There are these other disease processes that can lead to shock. 02:56 All right. 02:57 While we’re managing circulation, I already alluded to this before, but clearly if a patient has blood spurting out of a wound, you're gonna wanna apply some direct pressure to that to get that bleeding under control. 03:08 This is gonna be one of our immediate maneuvers that we do, during the primary survey to stabilize the patient. 03:15 In addition, we wanna make sure that our patient has adequate IV access. 03:19 This means two large-bore peripheral IV’s. 03:23 So you don't want just one, you want two, 'cause you wanna backup in case yours falls out or infiltrates. 03:29 You wanna make sure there are large bore, so that you can get a lot of fluid through them if you need to. 03:35 If you can’t get large bore peripheral access, you have other alternatives. 03:39 You can place an intraosseous line, or you can place a trauma line, which is a specialized central venous catheter that’s very large in diameter and allows large volume resuscitation. 03:53 When you do initiate fluid, you're always gonna start with isotonic crystalloid. 03:57 So generally, normal saline or lactated ringers for most patients. 04:01 Now every now and then, if you know upfront there was a large amount of blood loss, either because the patient is actively losing blood right in front of you or because the paramedics report that there was a lot of blood at the scene, you might consider going straight to blood transfusion, but generally, we're gonna start off with isotonic crystalloid and only move on to blood, if we don't got a satisfactory response from crystalloid. 04:25 Again, we're also gonna be looking for a specific injury patterns, and we’re gonna be providing treatments based on those underlying injuries. 04:34 We're gonna talk about tension pneumothorax and cardiac tamponade in future lectures. 04:40 So don't worry too much about that right now. 04:42 But understand that certain disease processes have specific treatments that you need. 04:48 You're not just gonna treat all hypertension or shock with fluid. 04:52 All right. 04:53 Moving on toward disability assessment. 04:55 So once we’ve covered A, B and C, the next thing we wanna think about is our patient’s neurologic status. 05:01 So we always wanna formally assess their level of consciousness. 05:05 The Glasgow Coma Scale is what’s used most commonly for this and we're gonna talk about that in some detail in our head injury lecture. 05:12 However, you can also use the abbreviated AVPU scale. 05:15 Which stands for alert, verbal, pain, or unresponsive. 05:20 Meaning, your patient is alert and normal, they respond only to verbal stimuli, they respond only to painful stimuli, or they’re completely unresponsive. 05:30 And as you can imagine, patients who only respond to pain or don't respond at all are clearly very ill and you should be very concerned about them. 05:40 While we’re doing our neurologic survey, we always wanna look at the pupils. 05:44 Pupillary function gives us a sense of whether the patient has a focal neurologic lesion or not. 05:50 We wanna look four extremity movement to make sure that there's not any evidence of neurologic focality that might suggest a brain or a spinal cord injury. 06:00 We wanna look for external signs of head or neck trauma, that may point us in the direction of a significant head her neck injury. 06:08 And lastly, if our patient is in any way shape or form altered, we wanna check their glucose. 06:14 Now clearly, trauma doesn't make you hypoglycemic, but remember, trauma is always precipitated by some event, right? And it’s not uncommon that people with medical illnesses will sustain trauma. 06:26 So if your patient became hypoglycemic that made them confused and then they crashed their car. 06:33 You know, clearly they're gonna have both the medical problem that precipitated the event as well as the traumatic injury for you to deal with. 06:40 So you wanna make sure that you're considering the big picture for your patient. 06:44 Checking their glucose, and checking other — for other signs of medical illness that might have contributed to the current event today. 06:52 All right. 06:53 There are a number of neurologic life threats that we’re looking for on our primary survey. 06:57 And we’re gonna talk in more detail about these in future lectures. 07:00 But these include any type of penetrating cranial injury, Intracranial hemorrhage, diffuse axonal injury and also high spinal cord injury, like C-Spine injuries. 07:13 In the realm of intracranial hemorrhage, we have a variety of different disease entities to think about. 07:19 We’ve got our subdural hematomas or epidural hematomas our traumatic subarachnoids and then lastly, intraparenchymal and intraventricular bleeding. 07:30 All of these are managed differently and we’re gonna talk about them in detail in the future lecture. 07:34 So what are we gonna do initially in our primary survey for patients who show signs of significant neurologic impairment? Well first and foremost, if their GCS is below eight, we wanna go ahead and intubate. 07:46 Patients who are significantly comatose are not gonna be able to maintain their own airways. 07:52 So it's very, very important that we manage the airway and make sure that the patient maintains a stable airway for the duration of their care. 08:02 We’re also of course gonna optimize their oxygenation and their perfusion. 08:07 So we're gonna be giving them supplemental oxygen. 08:10 If they’re intubated, we're gonna be placing them on a ventilator and we're gonna give fluids, blood, etcetera to ensure that they have adequate systemic perfusion. 08:19 We do wanna obtain emergent cranial imaging for any patient who has a significant neurologic disability on our evaluation, and the test of choice is really none contrast head CT. 08:30 But obviously, we’re not gonna initiate that until the patient is stable from an ABC perspective. 08:37 And again, there are specific disease entities that we’re looking for and how we manage those is gonna to vary depending on our CT findings. 08:46 So we’re gonna talk in more detail about how we would approach each one of these injury types as we move forward. 08:55 Lastly, after we've covered A,B,C and D, we wanna think about exposing the patient. 09:00 This is really, really important. 09:01 You've got to take all their clothes off, you’ve got to get all the coverings off. 09:05 You don't wanna miss any injuries, and I can't tell you how many times in my own practice I've seen injuries that are missed, because people don’t undress their patients. 09:13 So get the clothes off, get the sheets off, get a good look head to toe at the patient’s entire skin. 09:20 While you're doing that however, you wanna avoid hypothermia. 09:23 So hypothermia causes coagulopathy and exacerbates bleeding and trauma. 09:28 So you wanna expose your patient and look at them. 09:31 But once you've done that, get them covered up again, make sure you keep the room warm, make sure you use warm blankets, because trauma patients can actually become hypothermic very quickly. 09:40 Lastly, you’re gonna complete a head to toe exam. 09:43 So you wanna make sure that you look not only at the obvious stuff, but in the all the nooks and crannies. 09:48 You wanna look up in the axillae, in the perineum. 09:51 You wanna roll the patient over to examine the back obviously, while maintaining C-Spine immobilization. 09:58 And you wanna also make sure you get a look at the back of the head and the neck which is especially important in patient’s wearing cervical collars. 10:05 We often miss those if we don't remove the collar to examine the patient. 10:10 So take home points from this lecture, you’ve got to do a primary survey in all of your trauma patients, you’ve got to do it the same way every single time, so that you don't miss things, you got to be super systematic about this. 10:22 You wanna make sure that you look for specific life threats in the A, B, C and D domains. 10:30 And you wanna treat those as you identify them. 10:33 You wanna know the differential of consequence for A, B, C and D so that you know what you're looking for when you are doing your primary survey. 10:42 And if you follow these steps, you're gonna have a successful trauma resuscitation for all of your patients. 10:48 Thank you.
About the Lecture
The lecture Trauma: Circulation, Disability & Exposure by Julianna Jung, MD, FACEP is from the course Trauma (Emergency Medicine). It contains the following chapters:
- Circulation
- Disability
- Exposure
Included Quiz Questions
Which vascular pulse is the last to diminish in strength when circulation is compromised?
- Carotids
- Femoral
- Radial
- Dorsalis pedis
- Popliteal
What is the modality of choice for emergent cranial imaging?
- Non-contrast CT scan
- CT scan with contrast
- Non-contrast MRI
- MRI with contrast
- Cranial x-ray
Which circulatory life threat is the most common cause of death among traumatically-injured patients?
- Hemorrhagic shock
- Tension pneumothorax
- Cardiac tamponade
- Myocardial infarction
- Pericardial effusion
What is the management for tension pneumothorax?
- Needle decompression
- Orotracheal intubation
- Epinephrine administration
- Beta agonist administration
- Positive-pressure ventilation
Which of the following statements regarding the secondary survey of trauma patients is INCORRECT?
- Prevent hypothermia by exposing only significantly injured body areas.
- Include the axillae and the perineum in the secondary survey.
- To examine the back, roll the patient over to his side and secure neck immobilization.
- Cover the patient immediately once thorough examination is done.
- Do not forget to check the neck and nape area in patients wearing cervical collars.
A hypotensive patient with a systolic blood pressure of 60 will most likely only have a palpable pulse in what artery?
- Carotid
- Dorsalis pedis
- Popliteal
- Femoral
- Radial
Author of lecture Trauma: Circulation, Disability & Exposure

Julianna Jung, MD, FACEP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
systematic and very clear lecture with good explanation ,easy to digest
