Playlist
Show Playlist
Hide Playlist
Shoulder Region: Introduction

-
Slides Osteopathic Diagnosis of the Shoulder Region.pdf
-
Download Lecture Overview
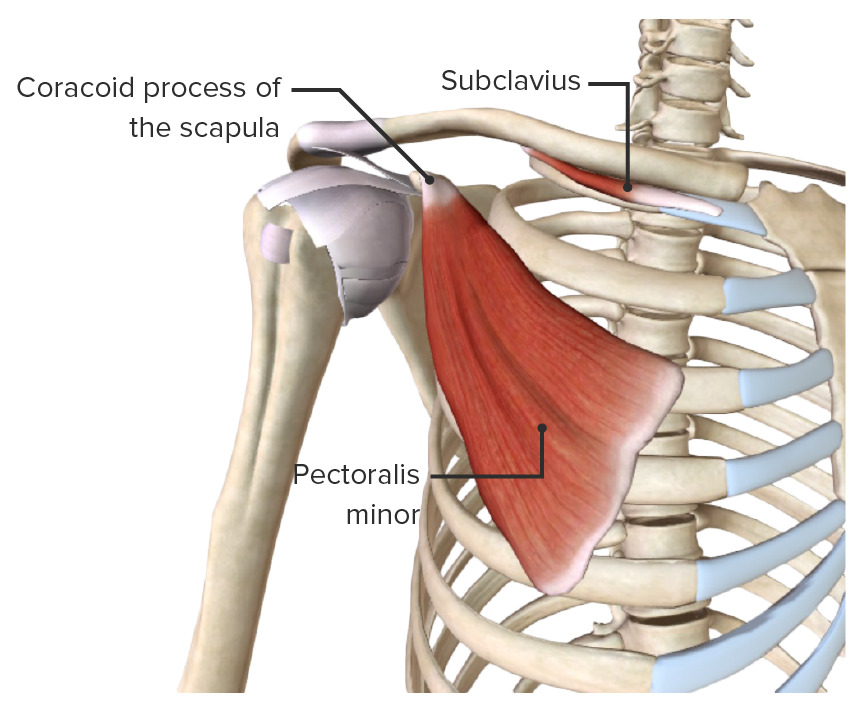
00:00 The shoulder joint is the most dynamic joint in our body. 00:04 Its flexibility allows us to have the freedom to perform many of our activities of daily living. 00:11 Integration of osteopathic diagnosis and treatment could help to address any sort of impairment that our patients may present with shoulder issues. 00:20 So let's take a closer look at the shoulder joint itself. 00:23 The joint consists of the articulation between the head of the humerus and the glenoid fossa of the scapula. 00:30 It is extremely mobile but at the same time, that makes it extremely unstable and more suspect to injury. 00:36 It is a ball and socket joint allowing for 180 degrees of potential motion and movement. 00:43 Our shoulder girdle consists of three bones: the clavicle, the humerus, and the scapula. 00:49 There are three true synovial joints: the glenohumeral, the sternoclavicular, and the acromioclavicular. 00:55 Then there are two functional joints, meaning that there's not an actual articulation of the bone to bone with a joint in between, but it's actually more of the motion and movement of the suprahumeral, meaning the space between the clavicle and the head of the humerus, and also the scapulothoracic, the functional joint of the scapula as it moves upon the thoracic cage. 01:18 There are ligaments of the glenohumeral joint that thickens into a capsule to try to provide support and keep that articulation between the head of the humerus and the glenoid fossa more secure. 01:29 The major support of the capsule are really the rotator cuff muscles. 01:33 The clavicle is an important bone to look at because this is the only bone that really stabilizes the shoulder to the midline skeleton. 01:42 The clavicle has two different joints: the acromioclavicular at the distal end and the sternoclavicular in the proximal end. 01:51 Again, the two major functions is to prevent the glenoid from turning anteriorly, and also protects different neurovascular structures that pass in the region. 02:01 Here's a closer look at the acromioclavicular and sternoclavicular joints. 02:07 If we have any sort of somatic dysfunctions that restrict the motion or movement at the A-C or S-C joints, it could potentially impact your shoulder mobility. 02:18 The scapula is located posteriorly along your thoracic cage. 02:25 It is a flat bone and it has some key important landmarks. 02:28 So you can note the spine of the scapula posteriorly where there are many muscle attachments. 02:33 The acromion process is the most distal portion of that scapular spine. 02:39 You have your coracoids process that juts anteriorly that you could find where the pectoralis muscles attach. 02:45 Then you have your glenoid fossa where the articulation between the humerus and the glenoid meet. 02:52 The humerus itself is the other side of the shoulder joint. 02:56 You have an anatomical neck, greater tuberosity there, and also a lesser tuberosity. 03:01 In between is a groove where the biceps tendon runs through. 03:07 The rotator cuff muscles help to stabilize the shoulder joint and at the same time help to move the shoulder joint. 03:14 So these four muscles are extremely important to remember. 03:17 We have the supraspinatus muscle which helps with shoulder abduction. 03:21 We have the infraspinatus and the teres minor muscle which helps with shoulder external rotation. 03:27 Then you have your subscapularis muscle which helps with internal rotation. 03:31 Again, these muscles help to stabilize the joint and also provide these motions at the shoulder joint. 03:37 A way to remember these muscles is SITS. 03:40 This is a mnemonic taking the first letter of each muscle, so the supraspinatus, infraspinatus, teres minor, and subscapularis. 03:46 If you take the first letter of each of these muscles, it spells out SITS. 03:50 So that's an easy way to try to remember your four rotator cuff muscles. 03:55 For shoulder joint motion and movement, there is an association between the humerus and the scapula. 04:03 For every 10 degrees of humerus abduction, there needs to be 5 degrees of scapula abduction because anatomically you cannot abduct the humerus without motion of the scapula coming out in abduction also. 04:16 Otherwise, it would compress the muscles and the neurovascular structures right above this humerus in the suprahumeral space. 04:25 Range of motion testing of the shoulder, we could motion test the shoulder in many different planes of motion. 04:31 Again, the shoulder is the most mobile joint. 04:34 So in the sagittal plane with flexion and extension, we should be able to flex the shoulder about 180 degrees and extend about 45 to 60 degrees. 04:42 In abduction and adduction in the coronal plane, we should be able to abduct our shoulder about 180 degrees and adduct about 45 degrees. 04:52 Internal and external rotation is a little bit harder to measure in the shoulder. 04:56 When we're measuring this motion at transverse plane, we could have the patient flex their elbow so that we could actually measure the number of degrees the shoulder is going to turn. 05:06 In internal rotation, if this is zero with our elbows stabilized next to our body, we could internally rotate our shoulder and we could also externally rotate our shoulder. 05:15 The key is to really stabilize the elbow joint so that you don't let the elbow move. 05:20 Otherwise, you may get a false reading based on your measurements. 05:25 The other way to measure internal and external rotation of the shoulder is to bring the arm up to 90 degrees and then have the patient slowly bring their arm, shoulder into internal rotation and into external rotation. 05:36 Again, it's good to stabilize the shoulder and the elbow as you're performing these range of motion testings. 05:43 If you have a restriction in range of motion testing, this will help you with diagnosis of a shoulder somatic dysfunction. 05:51 Remember, somatic dysfunction is a restriction of motion. 05:54 So when we find a restriction of motion in a particular plane, we're going to name that somatic dysfunction for its freedom of ease. 06:03 You don't want to confuse the diagnosis. 06:07 So what you're going to do is you're going to find a restriction of motion. 06:10 Let's say my shoulder is restricted in flexion. 06:14 I don't call it a shoulder flexion somatic dysfunction because somatic dysfunction is always named for its position of ease. 06:21 What I'm going to call it instead is it is a right shoulder restriction or a right shoulder extension somatic dysfunction, naming it the opposite direction. 06:32 These are the possible somatic dysfunctions of the shoulder based on the planes of motion and the motions that we have at the shoulder. 06:41 You could have a flexion or extension somatic dysfunction in the sagittal plane. 06:44 You could have an internal and external rotation somatic dysfunction in the transverse plane. 06:48 And you could have an abduction and adduction somatic dysfunction in the coronal plane. 06:53 Let's practice this information. 06:55 We have a 35-year old male, comes in with right shoulder pain after painting the ceiling yesterday. 07:00 On physical exam, you note that he could flex his right shoulder 80 degrees and his left shoulder 180 degrees. 07:06 What is the correct shoulder somatic dysfunction diagnosis? Here on motion testing, we note that the left shoulder has full range of motion at 180 degrees but the right shoulder is limited at 80 degrees. 07:22 So the right shoulder is the problem shoulder. 07:24 The problem is that there is limited right shoulder flexion. 07:28 So the somatic dysfunction is to call it for its freedom. 07:31 So this is a right shoulder extension somatic dysfunction.
About the Lecture
The lecture Shoulder Region: Introduction by Sheldon C. Yao, DO is from the course Osteopathic Diagnosis of the Shoulder Region.
Included Quiz Questions
Which of the following bones is responsible for stabilizing or attaching the shoulder girdle to the midline skeleton?
- Clavicle
- Humerus
- Sternum
- Radius
- Scapula
Generally, what is the normal range of motion for both flexion and abduction of the shoulder joint?
- 180 degrees
- 45 degrees
- 90 degrees
- 120 degrees
- 360 degrees
Abduction somatic dysfunction occurs when there is restriction of movement in which of the following anatomical planes?
- Coronal (or frontal) plane
- Sagittal plane
- Apical plane
- Transverse plane
- Horizontal plane
Author of lecture Shoulder Region: Introduction

Sheldon C. Yao, DO
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
