Playlist
Show Playlist
Hide Playlist
Renovascular Disease: Etiology and Pathophysiology – Secondary Hypertension


-
Slides Secondary Hypertension.pdf
-
Download Lecture Overview
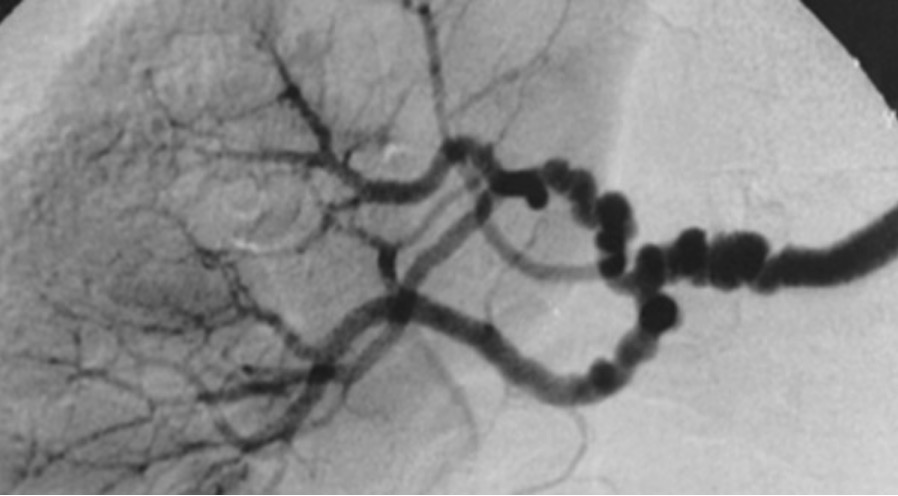
00:01 So, let's talk about renovascular hypertension which is what our patient has. 00:05 This is really defined by hypertension that's caused by renal artery stenosis or narrowing of the renal artery. 00:12 It could either be unilateral or bilateral. 00:16 If you'll look at the top image, this is a renal angiogram that actually shows a very tight stenotic lesion at the proximal takeoff of that left renal artery. 00:27 The lower image is another renal angiogram that actually shows bilateral renal artery stenosis, again, right at the takeoff or proximal part of the arteries. 00:37 The prevalence of renal artery stenosis is variable. 00:41 It really depends on the clinical circumstances. 00:44 So, for example, in patients who only have mild to moderate hypertension, it's less than 1% but in patients with severe or refractory hypertension, it's more in the order of 10-40%. 00:56 When we think about the different etiologies that cause renal artery stenosis, by far and away, the most common is atherosclerotic disease or atherosclerosis. 01:08 It causes about 75-90% of renovascular hypertension. 01:13 It's typically seen in patients who are over the age of 50 and they also have cardiovascular risk factors. 01:20 That means that they might be using tabacco, they have dyslipidemia, or peripheral vascular disease. 01:25 If you look at the image here to the right, this is a patient who has peripheral vascular disease, who has arterial insuffeciency characterized by cold diastolic extremities, arterial insuffeciency ulcers involving the lateral malleolus, and dependent rubor. 01:40 So, if that patient is sitting in front of me with hypertension, I'm definitely going to be suspect for renovascular disease due to atherosclerotic disease. 01:49 Now, the other one that I want you to keep in mind is fibromuscular dysplasia. 01:54 This is what our patient case had. This represents about 10-25% of renovascular hypertension. 02:01 It's a nonatherosclerotic noninflammatory vascular disease characterized by medial hyperplasia and involves nearly every arterial bed but most commonly, it manifest in the renal arteries, cervical arteries, vertibral and visceral arteries. 02:16 It presents between the ages of 30-50 years of age and women are more common than men to have fibromuscular dysplasia. 02:25 This is actually an image of a renal angiogram again and this is showing a very classic beads on a string appearance that is very suggestive of fibromuscular dysplasia. 02:36 So, other etiologies to think about that can result in renovascular disease are things like aortic and renal dissection, Takayasu's ateritis, this is a large vessel vasculitis that primarily affects the aorta and its branches, thrombotic or cholesterol emboli, this typically occurs when people have aortic manipulation, coronary artery or renal artery manipulation, and if you're doing something like percutaneous transluminal angioplasty or placing a stent, it's very easy to dislodge pieces of cholesterol. 03:08 They embolize distally to the arterial beds resulting in renovascular disease. 03:13 You can also have post-transplant renal artery stenosis. 03:17 This is typically due to people who are recepients of living donors. 03:22 It's the way that that kidney is actually anastomosed into the vasculature, there's a little bit of a bend at that anastamoses and that can result in renal artery stenosis. 03:33 And then post radiation, people who have had pelvic radiation can also result in renal artery stenosis. 03:39 So, why does this happen? What's the pathophysiology behind this? This is really due to reduced renal artery perfusion or decreased renal perfusion pressure. 03:49 That results from that stenotic lesion of the arterial vasculature in either one or both kidneys. 03:55 That decrease in renal perfusion pressure then activates the renin-angiotensin-aldosterone system or RAAS system. 04:02 That, of course, results in angiotensin II stimulation causing the following to result in sustained hypertension. 04:10 Increase in sympathetic nervous system activity, vasoconstriction of the blood vessels, antidiuretic hormone release which will cause water retention, and of course, aldosterone release from the adrenal gland causing sodium retention. 04:25 This is a schematic that diagrams exactly what we're talking about and again, illustrates the pathophysiology behind renal artery stenosis or renovascular disease. 04:36 So, what typically happens, remember we described that there's a decrease in renal artery perfusion pressure. 04:42 When that happens, GFR decreases. 04:44 That means less sodium chloride is delivered to the macula densa. 04:48 The juxtaglomerular apparatus then will secrete renin in response to that. 04:53 Remember, renin is responsible for cleaving angiotensinogen to angiotensin I. 04:59 Angiotensin I then gets converted to angiotensin II by angiotensin-converting enzyme in the pulmonary endothelium and then angiotensin II has multifactorial targets. 05:12 It's going to cause blood vessel vasoconstriction, it's also going to cause ADH release from posterior pituitary so that you'll have water retention by aquaporin channels being inserted into that collecting duct and reabsorbing water, and finally, aldosterone release from that zona glomerulosa in the adrenal cortex and that ultimately is going to cause sodium retention at that principal cell. 05:34 So, taken together, this patient has salt and water retention.
About the Lecture
The lecture Renovascular Disease: Etiology and Pathophysiology – Secondary Hypertension by Amy Sussman, MD is from the course Secondary Hypertension.
Included Quiz Questions
Which of the following is associated with fibromuscular dysplasia?
- A string of beads on a renal angiogram
- Elevated ESR and CRP
- Diffuse proliferative glomerulosclerosis on renal biopsy
- Anemia and thrombocytopenia
- Hyperkalemia
Which of the following is true regarding renal artery stenosis?
- Risk factors for atherosclerotic disease are often present.
- It is seen in about 10% of individuals with mild to moderate hypertension.
- It does not affect overall kidney function.
- Urinalysis frequently shows advanced proteinuria and RBC casts.
- It causes an inappropriate inhibition of RAAS.
Which of the following is associated with the pathogenesis of renovascular hypertension?
- Increased ADH release
- Increased sodium excretion
- Increased water excretion
- Decreased aldosterone release
- Widespread vasodilation
Author of lecture Renovascular Disease: Etiology and Pathophysiology – Secondary Hypertension

Amy Sussman, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
