Playlist
Show Playlist
Hide Playlist
Generalized Seizure in Children

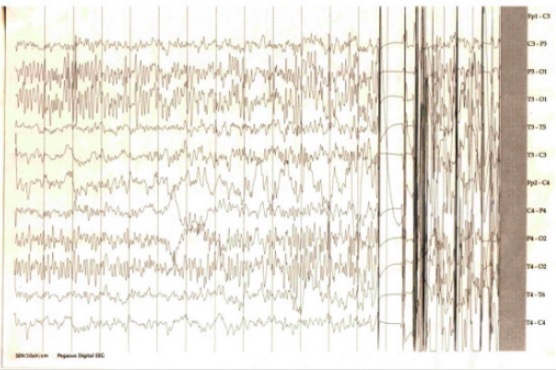
00:01 Let's move on to generalized seizures. 00:05 In a patient with generalized seizures, i it's important to control the seizure but you probably got about five minutes remember most pediatric seizures will stop of their own accord within five minutes. 00:18 An EEG after a seizure is done maybe useful for identiyfing underlying seizure syndromes. 00:25 Let me give you an example. 00:28 Lennox Gastaut Syndrome has an onset between typically three and five years of age. 00:34 These patients have mixed varieties of seizure and they may develop mental retardation. 00:41 And severe behavioral problems. 00:44 Lennox Gastaut has a very typical EEG pattern. 00:48 It is not so important for a medical student or a resident or even a fellow would probably need to know it if there is a neurology fellow. 00:58 But most of us don't really need to know how to read EEGs But we should be aware that there are certain patterns in them that give away certain diagnosis. 01:07 And Lennox Gastaut does have a typical EEG appearance. 01:11 The reason why it is important to make the diagnosis of Lennox Gustaut is because it is a difficult to manage disease and will require the guidance of a pediatric neurologist. 01:22 Here is an example of an EEG. 01:25 What you see here is a patient with Lennox-Gastaut You can here that there are intermittent periods of independent polywave spikes lasting for roughly one to eight seconds. 01:36 And that is classic and emblematic of that disease. 01:42 We've got Levetiracetam (commonly called Keppra), Dilatin or Phenytoin. 01:48 We've got Phenobarbital and Ethosuximide. 01:52 These are all drugs that we are going to use to place a child on all the time to help prevent them from getting recurrent seizures, when their seizures are frequent. 02:01 Keppra is our most commonly used drug, and we use it as a common first-line agent to prevent seizures in children, both with ongoing seizure disorders, and sometimes temporarily for a period of time after serious brain injury to prevent seizures from happening as a prophylaxis measure. 02:16 An important side effect of this med, especially in babies, is irritability, and this can be counteracted somewhat by providing Vitamin B-6 as well. 02:26 Other side effects can include diastolic hypertension and nausea or vomiting. 02:32 Dilantin is good for partial or generalized seizures. 02:37 The problem is you need to know the serum drug levels of the patients on this drug and over time they can develop side effects. 02:43 The side effects that you are going to be asked about on your tests is probably Gingival hypertrophy. 02:48 They get excessively growing gums around their teeth. 02:51 They also have increased body hair. 02:53 Usually in the arms you can see it very easily. 02:56 And long term, they can have neurotoxic effects with actually a loss of IQ points over time. 03:02 So in general we like to avoid seizure drugs unless we need them. 03:06 Phenobarbital generally used and better on children under one year of age, although it has been largely replaced by Keppra. 03:13 It is good for partial or generalized seizures, and again, we are going to have to follow drug levels. 03:19 This can cause a loss of IQ points over time. 03:22 It has a general sedating effect, which mitigates somewhat over time as they get used to the drug. 03:27 But be careful to warn the parents that for the next week or two, their child may be excessively sleepy. 03:33 Ethosuximide is our first line anti-seizure medicine for children with absence seizures. 03:38 So, I threw it in here as an alternative example of a seizure medication that you will see children being on. 03:43 The side effects of Ethosuximide are drowsiness, behavioral changes, nausea and they can get an Aplastic anemia or a lupus-like syndrome. 03:51 The general principle here is that there are lots of drugs we use in children we need to know what the side effects are and we need to know which drugs are most effective in which seizure syndromes. 04:01 It's really a matter of what the side effect profile what are your monitoring needs and what the seizure type is. 04:10 Let's switch goals to focal seizures. 04:14 Now remember, only children with focal seizures are going to have auras warning them of an impending seizure. 04:23 Auras are unique things for each child. Sometimes they will see certain colors or just get a sense that a seizure is coming on. 04:31 Focal seizures usually affect one area of the body. 04:35 Let's say an arm or a face. 04:37 The child may be fully awake during the event. 04:41 If we diagnose it with EEG, but an MRI is absolutely indicated in a child with a first time focal seizure because we need to rule out a focal abnormality in the brain. 04:53 We're going to treat focal seizures with AEDs, implanted devices and in bad cases, ketogenic diet or surgercal removal of the lesion. 05:04 Infantile spasms are a severe and very sad disease that happens to infants and can have terrible progrnosis. 05:16 These look really unique. 05:18 And I urge you to go online and get to Youtube and find a video of infantile spasms. They are all over the place. 05:26 It is important to be able to recognize them because diagnostically, It is important to make this diagnosis. 05:32 These children have generalized myoclonic jerks of the neck, trunk and limbs. 05:38 It generally begins between 3 and 7 months of age. 05:42 The specific etiology of the majority are unknown or they're genetic or syndromic. 05:49 Children who are not actively seizing will start off with having a normal neurologic exam and the typical EEG finding is something called hypsarrhythmia. 06:00 You should probably remember that that might show up on a test. 06:05 Infantile spasms have a very bad diagnosis. 06:08 And it is a very bad prognosis. 06:11 The death occurs for about 1/3 within 3 years of diagnosis. 06:15 These children have profound cognitive effects from their recurring seizures These seizures are profoundly hard to control. 06:22 and in survivors, they gradually turn into other types of seizures which can persist into adulthood. 06:31 Another type of seizure that is much less concerning is Benign Rolandic Epilepsy. 06:38 This is also called Benign Epilepsy with Centrotemporal spikes or BECTS. 06:45 That's because these patients tend to have Centrotemporal spikes on their EEG. 06:51 This present as several partial seizures usually in the face and in the hand. 06:56 It begins a little bit older between 5 and 12 years of age. 07:00 And usually with normal children who are developing normally. 07:04 What is key is they usually occur during sleep. 07:07 or within an hour of falling asleep. 07:11 Almost all are outgrown during adolescence. 07:14 They have those specific EEG findings, and treatment is optional because they are asleep while having the problem.
About the Lecture
The lecture Generalized Seizure in Children by Brian Alverson, MD is from the course Pediatric Neurology. It contains the following chapters:
- Generalized Seizures
- Focal Seizures
- Infantile Spasms
- Benign Rolandic Epilepsy
Included Quiz Questions
Which of the following statements is TRUE about infantile spasms?
- Hypsarrhythmia is seen on EEG.
- It typically presents with focal seizures.
- The typical onset is after 3 years of age.
- You usually note absent corpus callosum on MRI.
- Patients will have decreased deep tendon reflexes bilaterally.
Which of the following is NOT a feature of Lennox Gastaut syndrome?
- The patients have only focallized seizures.
- Onset is at the age of 3-5 years.
- Patients can develop mental retardation and behavior problems.
- The EEG shows the typical pattern of intermittent independent polywave spikes lasting 1-8 seconds.
- Management is difficult.
A mother brings her 8-year-old child to the clinic. She complains that her son performs poorly in school and his teachers always complain that he does not pay attention. On further questioning, the mother says that her son often stares blankly and becomes unresponsive for a few seconds several times a day. What is the drug of choice for this child?
- Ethosuximide
- Carbamazepine
- Lamotrigine
- Phenytoin
- Phenobarbital
Which of the following is a side effect of phenytoin?
- Increased body hair (hypertrichosis)
- Nausea
- Aplastic anemia
- Loss of IQ points
- Sedation
Which of the following is FALSE regarding focal seizures?
- The child will always lose consciousness during the attack.
- They have auras warning the occurrence of another seizure.
- An MRI is done to rule out a focal cause.
- It usually involves one area of the body.
- They can be treated with an implanted device.
Which of the following statements about Benign Rolandic Epilepsy (or Benign Epilepsy with Centrotemporal Spikes - BECTS) is TRUE?
- Its usual onset is at 5-12 years of age.
- EEG findings are non-specific.
- Treatment is very difficult
- It persists beyond childhood.
- Seizures are complex generalized.
Author of lecture Generalized Seizure in Children

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Great overview of the most important diseases to know and their features.
Very nice lectures with beautiful presentation that made me understand pediatric
