Playlist
Show Playlist
Hide Playlist
Osteopathic Evaluation of the Sacrum

-
01 Slides Osteopathic Diagnosis of the Sacral Region I.pdf
-
Download Lecture Overview
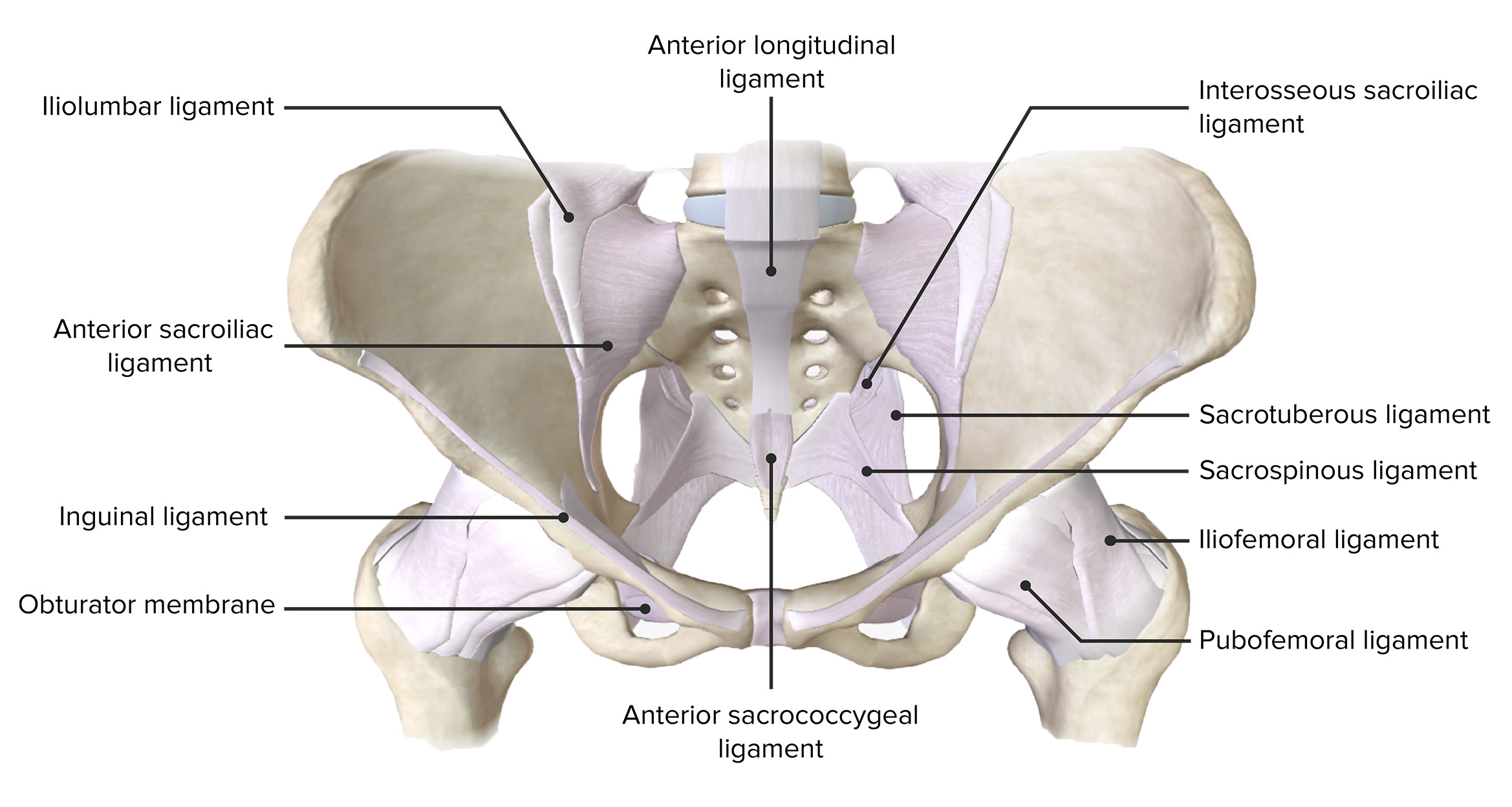
00:01 Start with the sacrum. 00:03 It's a saying every DO needs to know and every DO needs to practice. 00:08 So, we're going to talk about the sacrum, sacral mechanics, sacral disease, sacral dysfunction. 00:13 The reason being is number one, the parasympathetic connection to the organs; number two, the pelvic organs that are right there that are going to have some effect from it; number three, the fact that we do have to worry about it in trauma or surgery; and number four, the biomechanics of the pelvis. 00:30 It's a fulcrum. It's a keystone. 00:32 It affects how we hold our weight, how we function. 00:36 It's also a key to getting people better because once you've got the sacrum functioning, other things can function as well. 00:44 So, here is the sacrum. You're going to hear this a lot. 00:48 When I focus on the sacrum, I always start with the seated flexion test. 00:53 I look at the sacral sulcus, what's deep, what's anterior, and you look at the inferior lateral angle. 00:59 Those are the three tests you're going to do again and again. 01:02 But starting with the anatomy, here's the sacrum. 01:06 You get the top of the sacrum which is flat and attaches to L5. 01:11 Yes, there's a lot of connection. The whole body is connected. 01:15 L5 and S1 are going to affect each other's function. 01:18 But we're going to focus on the sacrum and the fact that you have the sacral promontory and that it is going to be anterior, connected. 01:28 I'll show you some pictures there. 01:30 I wanted to share a skeleton with you and show you the orientation of the sacrum in the skeleton because when you look at a normal skeleton that's hanging on a hanger, it tends to hang down and the pelvis tends to fall. 01:45 The sacrum looks like it's going straight down and it’s not. 01:49 You've got the quadratus lumborum. 01:51 You've got the large muscles that are pulling up the sacrum. 01:56 So, if you look at the picture from the anterior aspect, the sacrum is pulled up. 02:00 You have it attached to L5, pulled up with the coccyx coming down. 02:04 That's the orientation. 02:06 That's the way to look at the sacrum and to think about it. 02:09 The sacrum is tightly held into place with three large ligaments. 02:15 These are critical. Yes, the ligaments have synovial joints within them. 02:21 Yes, there's a joint between the sacrum and the ilium, ischium, and pubic symphysis. 02:28 The three bones of the pelvis that make up the innominate that connect to the sacrum do allow for some motion. 02:35 We will start springing it. We will start measuring it. 02:38 We will start assessing the symmetry of it. 02:41 But the sacrum itself is held together with the pelvis by three large ligaments. 02:47 First is the sacrotuberous from the sacrum to the ischial tuberosity, sacrotuberous. 02:56 The next is the sacrospinous. 03:00 That goes from the inferior lateral angle of the spine to the pelvic bone, the innominate. 03:07 I like to call it the ischium because there are lots of innominates. 03:10 But that's the second large one is sacrospinous. 03:14 The sacrospinous ligament is going to create a greater and a lesser sciatic foramen. 03:21 So this is clearly demonstrated here. 03:23 If you look above, you'll see the greater; if you look below, you'll see the lesser sciatic foramen. 03:29 The third large ligament is the iliolumbar ligament. 03:34 The iliolumbar ligament goes from L4, L5 and it attaches to the iliac crest. 03:43 It's often where you see a lot of pain, a lot of problems particularly when there's a lumbosacral dysfunction that's occurring. 03:51 Here is another picture of the bones and ligaments of the pelvis. 03:55 So you can see the orientation. 03:57 You can see the connection because we often test the sacrotuberous ligaments. 04:03 Push on them. See the laxity. Make sure of the symmetry. 04:07 There are other ligaments on top of it and on the side of it you’re going to have to focus on as well, particularly when things don't make sense. 04:13 Here's just a photo showing the synovial portion of the sacroiliac joint. 04:21 Because when you look at the ligaments, you think that they should be attached and not moving but they are moving. 04:27 There is synovial fluid in there and there is more motion. 04:31 The sacrum is also stabilized through long muscles. 04:37 Longissimus spinalis and iliocostalis go more than two spinal segments and will come down and attach to the sacrum. 04:47 The multifidus and rotatores, small segments, still keep the motion, stabilize the body. 04:53 Both are small muscles that go one to two segments. 04:55 The large muscles are important and contribute to the stability of the sacrum. 05:00 Again, the sacrum absorbs the weight of the body and splays it so it's supported by both the pubic bones and the hips. 05:09 So, that's one of the key aspects of the sacrum. 05:13 Here is another photo of the muscles, the gluteus medius, minimus, piriformis and their attachments to the sacrum. 05:22 Piriformis is one we focus on quite a bit because there's a lot of problems with it, a lot of pain that's associated with it. 05:31 Piriformis causes external rotation and extension of the thigh. 05:36 It also causes abduction. 05:39 It's supplied by S1 and S2 and it's a common place where we see pain and problems. 05:45 Piriformis syndrome is something we assess for often. 05:48 Another picture of the sacrum. 05:50 Here you can see the sacral promontory where L5 is going to attach. 05:54 At the bottom where you have the sacrum attached to the coccyx is another connection point. 06:02 The sacrum is typically fused by 18 years of age in men, 21 years of age in women. 06:08 It's normally four to six sacral vertebrae that fuse and form one sacral bone. 06:16 Then it attaches to the coccyx which has three to five segments to it. 06:21 Once it's solidified by 30 to 40 years of age, you're not going to have further motion of the bones in and of themselves but you will have motion where they connect to other bones. 06:33 The lumbosacral junction, the angle between L5 and S1, also called Ferguson's angle is important because if it's less than 25 or more than 35, you have to worry about increased issues with the connection. 06:48 You have to worry about more pain. 06:50 You can have an increased lumbar lordosis when the angle is greater. 06:54 Then people aren't going to be able to function as smoothly. 06:57 So, measure the angle. If it's between 25 and 35, it decreases the suspicion for lumbosacral pain and gets you feeling that the body can heal itself. 07:07 If it's greater, you worry more about spondylolisthesis, spondylosis and other abnormalities. 07:14 Here is a picture of the sacrum which is L-shaped. 07:17 It gives you a sense of the motion of L5 on S1. 07:21 It shows you where the angle occurs and why you're worrying about it, as well as the zygapophysial joint that's connecting the two. 07:28 We're going to go to the three transverse angles, anatomic angles that will tell you where some of the motion is going to occur. 07:37 When we look at people, we look mostly at them obliquely. 07:42 That's because when you walk, right on right oblique angle, left on left oblique angle occurs with each step. 07:48 That's normal physiologic functioning. 07:52 However, if you look at the anatomic functioning and where the anatomy makes it easy for motion to occur, it's going to be the superior transverse angle which you're going to see with craniosacral motion and respiratory motion. 08:07 You're going to see the rocking of the sacrum along the superior transverse angle. 08:13 The middle transverse angle, which is somewhat anteriorly, is going to move with posture. 08:20 So, as people rotate and try and find the posture, it's the middle transverse axis where the motion is occurring. 08:29 The inferior transverse axis much lower is where you have innominate rotation and where we're going to be monitoring for the inferior lateral angle to make sure that it's equal.
About the Lecture
The lecture Osteopathic Evaluation of the Sacrum by Tyler Cymet, DO, FACOFP is from the course Osteopathic Diagnosis of the Sacral Region.
Included Quiz Questions
Which of the following parts of the superior portion of the sacrum extends anteriorly and forms the posterior margin of the pelvic inlet?
- Sacral promontory
- Transverse ridges
- Anterior sacral foramina
- Apex
- Coccyx
Which of the following sacral ligaments, attaching the sacrum to the spine of the innominate bone, divides the greater and lesser sciatic foramina?
- Sacrospinous ligament
- Sacrotuberous ligament
- Iliolumbar ligament
- Posterior sacroiliac ligament
- Anterior sacroiliac ligament
Which of the following sacral ligaments, attaching the sacrum to the medial iliac crest, is often painful in patients with lumbosacral decompensation?
- Iliolumbar ligament
- Sacrospinous ligament
- Sacrotuberous ligament
- Posterior sacroiliac ligament
- Anterior sacroiliac ligament
Which of the following gluteal muscles that originates from the anterior sacrum may cause pain radiating to the posterior thigh as a result of impingement of the sciatic nerve?
- Piriformis
- Gluteus maximus
- Quadratus femoris
- Gluteus minimus
- Obturator internus
Which of the following sacral axes moves/changes with gait or postural changes?
- Middle transverse axis
- Superior transverse axis
- Inferior transverse axis
- Left oblique axis
- Right oblique axis
Author of lecture Osteopathic Evaluation of the Sacrum

Tyler Cymet, DO, FACOFP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
