Playlist
Show Playlist
Hide Playlist
Acne Vulgaris

-
Slides Dermatology Inflammatory Skin Diseases.pdf
-
Download Lecture Overview
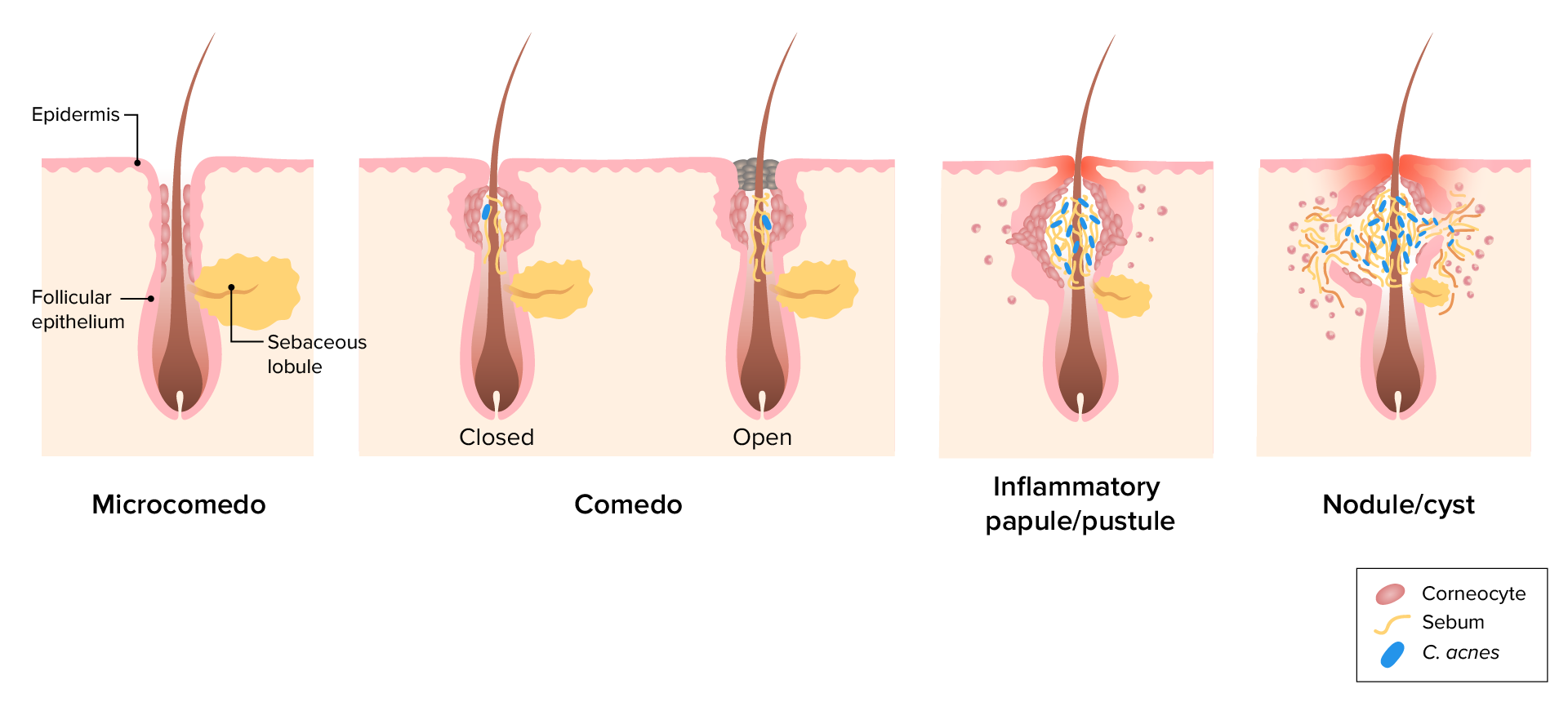
00:01 Our first topic is going to be one of the most common dermatologic presentations that we find in United States. 00:08 Many of us have gone through this, especially during puberty. 00:11 Our topic, obviously, being acne vulgaris. 00:14 Now, the acne vulgaris here that you’re seeing could be of different types. 00:18 You could have pustules, you could have vesicles. 00:20 So, in terms of description, it could be all over the place. 00:23 And notably, as I said, we talked about pathogenesis. 00:26 We’ll be focusing upon the puberty years. 00:31 Demographics: 80% of people seek medical care for acne in life. 00:36 Take a look at this pie; 80% with acne vulgaris with demographics. 00:41 It’s the most common found in teens and early adulthood. 00:45 So, you’re thinking about those pubertal ages. 00:48 Let’s take a look at etiology. 00:50 It’s multifactorial. 00:52 Here, as soon as you hear about acne vulgaris, it’s a fact that you’re thinking about your androgens playing a role. 01:00 Hence, andrenarche increases sebum production. 01:03 Think about your patient, a teenager, perhaps, going through puberty. 01:07 And so therefore, at this point, there is going to be increased levels of hormones, especially our androgens. 01:14 So, during andrenarche, increases sebum production. 01:19 Next, what happens? Well, then you had these comedones. 01:22 What’s a comedone? A comedone is basically the type of lesion that you expect to see with acne. 01:29 Now, you’ve heard of blackhead and white head. 01:31 And if it’s a blackhead, this would then mean that the comedone, so think about the lesion that occurs and think of this kind of being like a volcano, please, and that would be the best description here. 01:40 And if you’ve heard of blackhead, that basically means that here, the volcano has erupted, in other words, the comedone is now exposed. 01:48 So, the overlying skin or the cover has been now removed. 01:52 Once it’s removed, the inner contents of your comedone then gets exposed to the environment resulting in oxidation. 02:02 This oxidation then causes what’s known as blackish discoloration, and you call this a blackhead. 02:08 Whereas a whitehead, as you can imagine, the skin then is intact over the comedone. 02:13 And if it is intact, then please understand what then appears upon gross examination is going to be a whitehead. 02:21 So, comedone forms due to accumulation of lipid and keratin in the follicular unit, okay? So, think about where you are, maybe perhaps on your face, and you have a follicular unit, which is now undergoing this type of accumulation of lipid and keratin. 02:39 An important point here would be bacteria known as propionibacterium acnes. 02:46 The particular bacteria that you want to make sure that you memorize overgrow in abundance of such “oil”. 02:52 And by oil, what are you referring to? That sebum and lipid accumulation within your comedone. 02:59 The bacteria convert the sebum into fatty acids that elicited an inflammatory response. 03:05 And as soon as you think about inflammatory response, then you know that you have your WBC such as neutrophils that are going to come in. 03:13 All part of your etiology pathogenesis acne vulgaris. 03:19 Let’s talk about the morphology. 03:22 If you have an open comedone, what does that mean to you? Remember, you have that lesion that you’re looking for. 03:27 And instead of it being covered, it is now open. 03:30 So therefore, the overlying skin or epidermis is not intact, it’s open. 03:37 Once this type of exposure is taking place, the inner content of your particular lesion is now at risk for oxidation. 03:45 Now, what is it going to do? It will oxidize your keratin plug, and therefore, the coloration that it then gives or provides is a blackhead. 03:54 Whereas, if the epidermis over the comedone remains intact. 03:58 So now you have a papule without the oxidation because now you don’t have such exposure. 04:04 And therefore, upon gross examination, it appears being white. 04:08 Now, you could have acne vulgaris in which, unfortunately, it might get a little bit bigger. 04:12 And so therefore, now you’re thinking about a nodule. 04:15 And this will then arise from the follicle, rupture, and may then cause an inflammatory type of dermis. 04:21 You’re getting the dermis involved with nodules. 04:24 Then you have a more serious type of acne vulgaris. 04:27 You can call it nodulocystic lesion. 04:29 And this can then yield a systemic symptom, most often seen with teenager boys or teenagers that are males. 04:41 Management: Topical antiseptics. 04:45 Here, you want to memorize benzoyl peroxide. 04:49 So here, what you want to do is try to then make your particular “infection,” if you want to call it as such. 04:57 Remember, bacteria could also be involved. 04:59 And so therefore, you try to keep things as sterile as possible. 05:03 Antiseptics, it prevents the comedones, and perhaps, decreases bacterial count. 05:10 Oral antibiotics. 05:11 Example, tetracyclines. 05:13 Also, it depends on anti-inflammatory properties. 05:17 Most commonly, doxycycline, may cause photosensitivity. 05:21 Keep that in mind. 05:22 Or minocycline that may cause a drug-induced lupus. 05:26 Keep that in mind for this type of tetracyclines. 05:30 All tetracyclines can cause a condition or an adverse effect known as pseudotumor cerebri. 05:38 Remember, this is a patient that is then going to present with headaches, and there would be measurement of increased intracranial pressure. 05:47 Upon fundoscopic examination, there would be papilledema. 05:50 On imaging study, there would be nothing because this is a pseudotumor. 05:54 We talked about this earlier. 05:58 Continue our discussion of management. 06:00 Here, we have our vitamin A derivatives. 06:03 In other words, retinoids, and we have tretinoin as being a drug. 06:08 Prevents a comedone and may decrease the inflammation. 06:11 Oral retinoid, known as isotretinoin, reserved for severe nodulocystic scarring acne. 06:19 Remember now, you’re talking about a nodule that has also taken on a cystic type of appearance and could also have systemic involvement. 06:27 Remember those young teenage boys we were talking about most commonly may be seen with. 06:34 Now, with that, you need to make sure that you have minimal type of scarring taking place. 06:43 Something that you want to keep in mind with side effects. 06:45 It is, as you know with the retinoids, a huge teratogen. 06:50 Here also, as your tetracycline, pseudotumor cerebri could be a possible side effect, SE. 06:58 Hyperlipidemia because of accumulation of lipid. 07:01 Now, keep all this in mind when dealing with retinoids. 07:05 And with tetracycline, the common denominator between the two drugs is an adverse effect, pseudotumor cerebri. 07:16 As a differential diagnosis now, what we will do as we go through dermatology is rule things in or rule things out. 07:23 So at this point, our topic is still acne vulgaris. 07:27 Many of your skin conditions would be -- well, they might look quite similar, huh? And so therefore, what kind of things you want to know about as clinical pearls so that you can either rule things in or rule things out? Our topic here would be differential diagnosis of acne vulgaris. 07:42 A differential diagnosis. 07:44 Our topic here is acne rosacea. 07:47 I emphasized rosacea, not acne vulgaris but acne rosacea. 07:53 Well, how do you know if a patient has a rosacea versus vulgaris? Usually, with the rosacea, adult of Northern European heritage, maybe perhaps, Scandinavian. 08:03 You’re going to look for a patient that has particular triggers such as stress, spice, so on and so forth. 08:11 Then, there is going to be erythema, and specifically, the flushing that you’re going to find on the face, and hence, the differential with vulgaris. 08:21 There is going to be a background erythema, which is redness, but that’s nonspecific. 08:26 But then you have telangiectasia. 08:29 We’ll talk more about rosacea, and when we do, we’ll talk about something called rhinophyma. 08:33 And basically, you have a bulbous nose with rosacea and could also be associated with alcoholism. 08:41 Not always, huh? Not always. 08:43 And comedone is not a feature of rosacea. 08:47 Our topic, differential diagnoses of acne vulgaris. 08:51 Here are some clinical pearls so that you know that you’re dealing with rosacea versus vulgaris. 08:59 Other differentials: perioral/periocular dermatitis. 09:03 These would occur in specific areas and may follow topical steroid use. 09:08 Here, we have monophormic in its appearance, and inflammatory papules without comedones. 09:13 Once again, comedone would be more as high in your differential, either blackhead or whitehead as being acne vulgaris in that teenage population, and you’re looking for andrenarche type of issues, right? Here, comedone is not present with your dermatitis of periocular or perioral type of lesion. 09:35 A differential diagnosis for vulgaris would also be folliculitis. 09:39 Allow the name to speak to you. 09:41 So, we’re talking about the follicular unit, right? And with the follicular unit, you know that there is hair that is being also expressed. 09:47 So therefore now, the follicle or the follicular unit is undergoing infection, the hair follicle. 09:53 And related, in many respects, absolutely. 09:56 Now, could you have follicle involvement with acne vulgaris? Sure, you could. 10:01 But with folliculitis, specifically, is an infection, predominantly, on the trunk and extremities. 10:07 So, it doesn’t have to be on the face with folliculitis. 10:10 Occurs at any age, any age. 10:13 May progress to what’s known as furuncles, carbuncles, and abscesses. 10:17 Topics that we’ll take a look at in due time. 10:20 But at this point, please know that folliculitis, if not properly addressed, may go on to develop furuncles, carbuncles, or perhaps even, abscesses of that entire region.
About the Lecture
The lecture Acne Vulgaris by Carlo Raj, MD is from the course Inflammatory Skin Diseases.
Included Quiz Questions
What patient group is most commonly affected by acne vulgaris?
- Adolescents
- Infants
- Toddlers
- Postmenopausal women
- Elderly men and women
Which of the following pathogens is most commonly associated with acne vulgaris?
- Propionibacterium acnes (now called Cutibacterium acnes)
- Corynebacterium spp.
- Staphylococcus aureus
- Trichophyton rubrum
- Epidermophyton spp.
Which of the following medications is least commonly used to treat acne vulgaris?
- Trimethoprim-sulfamethoxazole
- Isotretinoin
- Benzoyl peroxide
- Doxycycline
- Minocycline
Which of the following medications used to treat acne vulgaris would be the safest during pregnancy?
- Benzoyl peroxide
- Doxycycline
- Minocycline
- Isotretinoin
- Tretinoin
Which of the following skin conditions is most similar to acne vulgaris in its mechanism and site of origin?
- Folliculitis
- Acne rosacea
- Periocular dermatitis
- Cellulitis
- Seborrheic dermatitis
Author of lecture Acne Vulgaris

Carlo Raj, MD
Customer reviews
3,1 of 5 stars
| 5 Stars |
|
3 |
| 4 Stars |
|
1 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
3 |
really well explained, repetition really helps the knowledge stick. explaining rather than just reading off the screen really helps swell
NICE LECTURE, short and understandable. feels like information is not enough. anyway, it's a good lecture. thank you, doctor Carlo.
Engaging presenter. Love the reinforcements of what is important to remember. Love that he includes DD and why those other DD can be ruled out. His lecture will stick.
Difficult to understand. Annoying accent. Difficult to concentrate on the lecture due to his presentation style.
