Playlist
Show Playlist
Hide Playlist
Antipsychotics

-
Slides Pharmacology Antispychotics.pdf
-
Download Lecture Overview
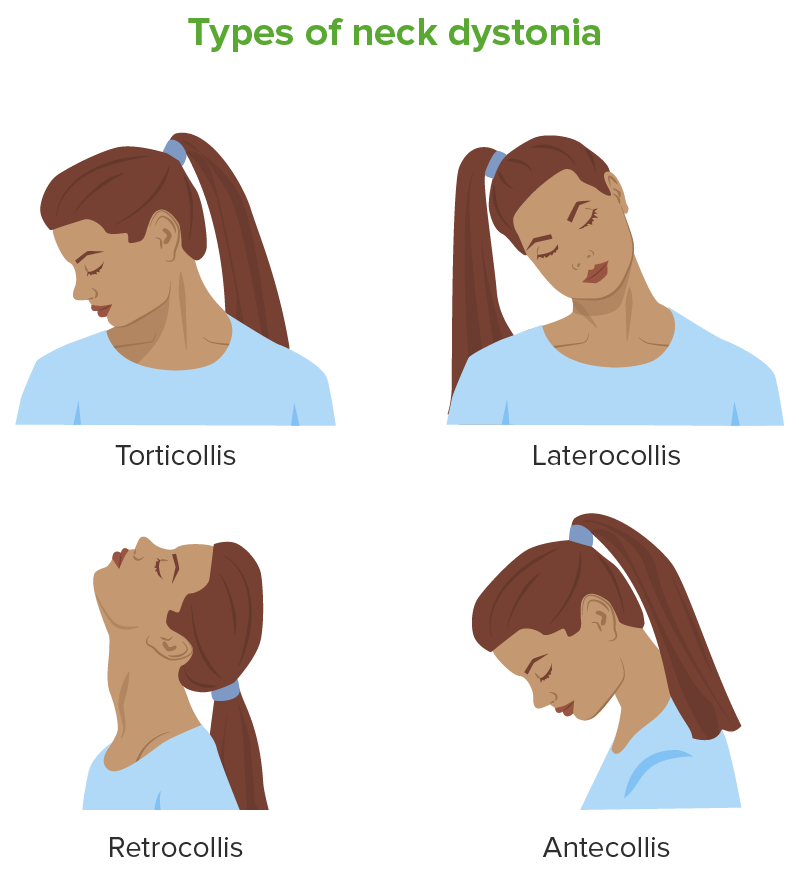
00:01 Antipsychotic treatment in pharmacology is an important topic. 00:05 Let’s go over the highlights here. 00:07 So antipsychotics are medications also known as neuroleptics, and they are categorized in terms of typical and atypical. 00:16 They work by blocking dopamine receptors and thereby reduce psychotic symptoms. 00:22 These are used to treat psychotic disorders, and also, psychosis that goes along with other disorders. 00:28 So throughout the lecture series, you’ve learned that psychosis can actually appear as a symptom of severe depression. 00:36 It can also come up during times of dementia. 00:39 So there are a lot of uses for antipsychotics and they can occur in other patients who don’t only have a primary psychotic disorder as well. 00:49 So let’s go through the two types, typical and atypical. 00:53 Well, examples of typical neuroleptics include chlorpromazine, thioridazine, haloperidol. 00:59 Atypical examples are things like risperidone and ziprasidone. 01:03 So, the typical neuroleptics, these are D2, dopamine 2 antagonists. 01:08 They have a pretty high potency. 01:11 Now, atypical neuroleptics do antagonize dopamine 2. 01:15 However, they’re lower potency for that and they actually also will target serotonin and histamine receptors as well. 01:23 The typical neuroleptics tend to be really good at treating positive symptoms. 01:28 But the atypicals are actually better at treating the negative symptoms, which we think of as the core of the psychotic symptoms. 01:35 Typical neuroleptics, because of their dopamine blockade, they can really cause a lot of extrapyramidal side effects. 01:43 That doesn’t happen as much with the atypical neuroleptics. 01:46 However, these are more likely to cause side effects like sedation, and also, weight gain or metabolic problems. 01:53 When it comes to the typical neuroleptics, there are again two subtypes. 01:58 There’s the high potency typical neuroleptics, and also, low potency typical neuroleptics. 02:04 So we’ll talk a little bit more about those later. 02:07 And for the atypical neuroleptics, as I said before, these tend to not only block dopamine but they also have a strong affinity for serotonin, alpha receptors, histamine receptors as well, and serotonin. 02:21 So, the antipsychotics, basically, again, this targets dopaminergic neurons. 02:26 That’s really the key, and there are few different dopamine pathways that you should be familiar with; the nigrostriatal, the mesolimbic, and the tuberoinfundibular. 02:37 Now, neuroleptics are highly fat soluble, and therefore, there are a lot of options for giving these intramuscularly or through an injection. 02:46 We’re going to review that later, but as a teaser, it’s important to know that when it comes to taking an antipsychotic medication, sometimes, patients are very agitated in the hospital setting and it’s really nice to have the option to do an injection of medication. 03:02 Likewise, some people don’t like taking a pill every day, and the long acting injectable antipsychotics actually allow for bi-monthly or monthly dosing, which can be a nice option for patients. 03:15 So there are a lot of different uses for antipsychotic medications. 03:19 Some are, of course, the primary psychotic disorders, also mood disorders like mania and depression, and Tourette’s syndrome. 03:26 They can also be helpful there. 03:28 So, let’s talk a little bit more about the typical antipsychotics, and let’s start with the low potency one. 03:34 These have a little bit of a lower affinity for the dopamine receptor. 03:39 And examples include chlorpromazine and thioridazine. 03:43 Now, there’s a higher incidence of anticholinergic effects with these medications, and a lower incidence of the extrapyramidal side effects that can be very upsetting to patients, also a little bit of a lower incidents of neuroleptic malignant syndrome, which can be a deadly side effect of antipsychotic medication. 04:01 The high potency typical antipsychotics have a very high affinity for dopamine blockade. 04:07 These include haloperidol, fluphenazine, and some other examples listed here. 04:12 There’s a very high incidence of EPS or extrapyramidal symptoms with these medications, and also, neuroleptic malignant syndrome; lower incidence of anticholinergic and antihistamine problems. 04:27 So, what are actual extrapyramidal side effects? You might be wondering, “Is this very important to know for your boards?” Extrapyramidal side effects come from dopamine blockade, typically through that nigrostriatal pathway. 04:40 And the earliest signs of this can be acute dystonia. 04:43 Now, this might manifest in your patient as something like an oculogyric crisis where their eyes kind of roll up in their head. 04:51 It can also be seen as torticollis or neck stiffness. 04:55 And acute dystonia can be very distressing to a patient, and it can occur immediately or within hours. 05:02 Next, another EPS symptom is bradykinesia or parkinsonian symptoms. 05:08 So this can look like masked facies where somebody doesn’t have a lot of expression. 05:14 It can also look like cogwheel rigidity, which you might test for when you’re doing your physical exam on a patient. 05:20 Some patients have this bradykinesia or slowed movements. 05:25 And they also can have a gate where they do something, which is called turning on block, meaning that they will make a sudden stop and then turn their whole body. 05:35 So it’s not very easy for them to shift in maneuver as it is for the rest of us. 05:40 They may also get a tremor which can be a cardinal feature of a Parkinsonian side effect from this medication. 05:47 Another problem that can occur within months of starting an antipsychotic medication is akathisia. 05:53 This is highly distressing to patients. 05:55 So, what akathisia is is it’s an internal sense of restlessness. 06:00 It will often manifest as a patient pacing, maybe tapping their foot or their hand on their leg. 06:08 They’ll often describe to their doctor that they just feel like they want to crawl out of their skin. 06:13 So, that’s a sign of akithisia, which again is very distressing. 06:18 And then a really important side effect of antipsychotics to know about is tardive dyskinesia. 06:24 Now, it can take years and even decades for a patient to develop tardive dyskinesia. 06:28 A little pearl for your exam is that elderly Caucasian women are at highest risks for developing tardive dyskinesia when they’re treated with an antipsychotic. 06:39 So what this actually looks like is abnormal movements for example of somebody’s face. 06:45 You may see someone sticking their tongue out repeatedly or smacking their lips together. 06:49 This can also occur less frequently in extremities or truncal areas. 06:54 And the really unfortunate thing about tardive dyskinesia is that in most cases, it’s actually not reversible. 07:01 So it can be very permanent and a disfiguring side effect. 07:05 Both traditional and atypical neuroleptics have similar efficacies in terms of treating positive symptoms of psychosis. 07:15 And you might remember the positive symptoms of psychosis or things like delusions, hallucinations, bizarre behaviors. 07:23 However, when it comes to treating the negative symptoms of psychosis, things like having a flat affect, little motivation, poor energy, speech alogia, that’s better treated with one of the newer antipsychotics or atypical antipsychotics. 07:42 So the traditional antipsychotic side effects to review them are antidopaminergic, anti-HAM, which we’ll go over that in more detail in a minute, and of course, tardive dyskinesia, in dystonia, or in other words, the EPS symptoms, including bradykinesia and akathisia, neuroleptic malignant syndrome, which we’ll talk about in more details, is also a serious side effect. 08:05 So in terms of tardive dyskinesia, we talked about it before but another little pearl to know, this is writhing movements of the mouth and tongue. 08:14 when your patient is described as having that, think tardive dyskinesia. 08:18 The antidopaminergic side effects are of course the extrapyramidal symptoms. 08:23 Also, hyperprolactinemia, and this is due to interference of dopamine in the tuberoinfundibular pathway. 08:31 So patients can actually end up with so much dopamine blockade that they get a surge in prolactin, and this can manifest as actually lactation from the breast, and it can occur in women, but also in men. 08:43 And the neuroleptic malignant syndrome is another very noteworthy side effect to look out for. 08:49 So I mentioned anti-HAM side effects before. 08:52 Let’s talk about what that means. 08:53 So the H is antihistamine, where patients can become very sedated. 08:58 The A is anti-alpha adrenergic side effects. 09:01 This can look like orthostatic hypotension, cardiac arrhythmias and sexual dysfunction. 09:07 The antimuscarinic side effects include dry mouth, tachycardia, urinary retention, blurry vision, and constipation, all things that are of course undesirable to your patient. 09:20 They may also get weight gain, elevated liver enzymes. 09:23 They may have eye problems or ophthalmologic problems, dermatological problems, and seizures. 09:30 And because tardive dyskinesia is so incredibly important and a potentially irreversible and disfiguring side effect, we’re mentioning it a lot here. 09:40 It’s really important to know about for your exam. 09:42 And it’s really important to note that it can lead to that permanent disfiguration. 09:47 If you have a patient showing signs of tardive dyskinesia, you really want to consider lowering their dose of antipsychotic, giving them a drug holiday from their antipsychotic or switching them to another agent, preferably, and atypical antipsychotic.
About the Lecture
The lecture Antipsychotics by Helen Farrell, MD is from the course Schizophrenia and Thought Disorders. It contains the following chapters:
- Antipsychotics
- Traditional Antipsychotics
- Tardive Dyskinesia
Included Quiz Questions
Which of the following drugs is better at treating positive symptoms in a psychotic disorder?
- Haloperidol
- Ziprasidone
- Risperidone
- Aripiprazole
- Olanzapine
A patient presented to the clinic with acute onset of muscle spasms, stiffness and upward deviation of the eyes 6 hours after initiating treatment for psychosis. Which of the following drugs is the most probable cause for his presentation?
- Trifluoperazine
- Quetiapine
- Bromocriptine
- Risperidone
- Olanzapine
Which of the following pathways is responsible for the extrapyramidal side effects of antipsychotic drugs?
- Nigrostriatal
- Mesolimbic
- Tuberoinfundibular
- Cortico-basal
- Mesocortical
Which of the following groups are at the highest risk for developing tardive dyskinesia when treated with an antipsychotic?
- Elderly Caucasian women
- Young African American men
- Elderly American Indian women
- Elderly Asian women
- Young Hispanic men
A patient on haloperidol for the past 4 years presents with constant lip-smacking and tongue protrusion. You conclude that the patient has tardive dyskinesia. Which of the following is NOT a therapeutic option to treat the patient's current complaint?
- Adding clozapine
- Lowering the dose of the antipsychotic
- Switching to ziprasidone
- Switching to olanzapine
- Giving a drug holiday to the patient
Author of lecture Antipsychotics

Helen Farrell, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I like very much because is very well explained and very organised.. It contains all necessary and important information about anti-psychotics
