Playlist
Show Playlist
Hide Playlist
Hypopituitarism


-
Slides AnteriorPituirary EndocrinePathology.pdf
-
Download Lecture Overview
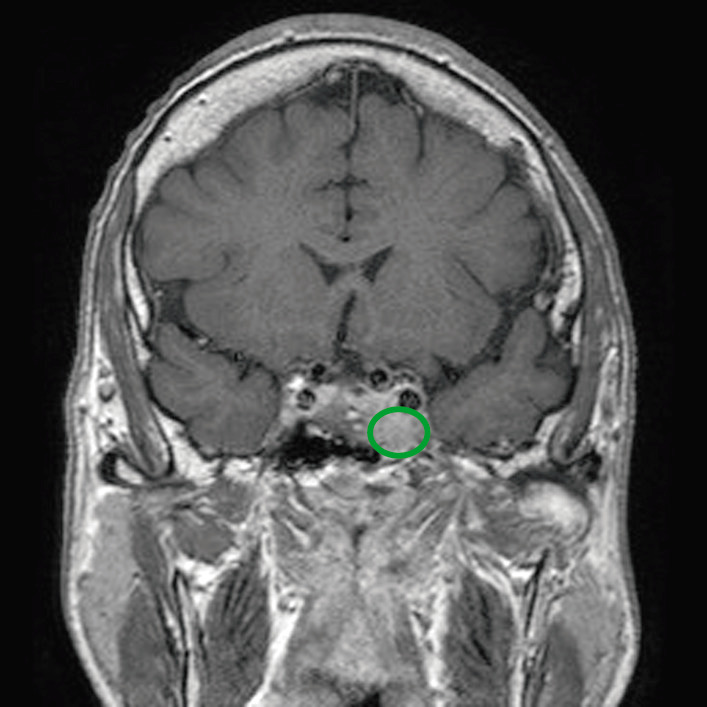
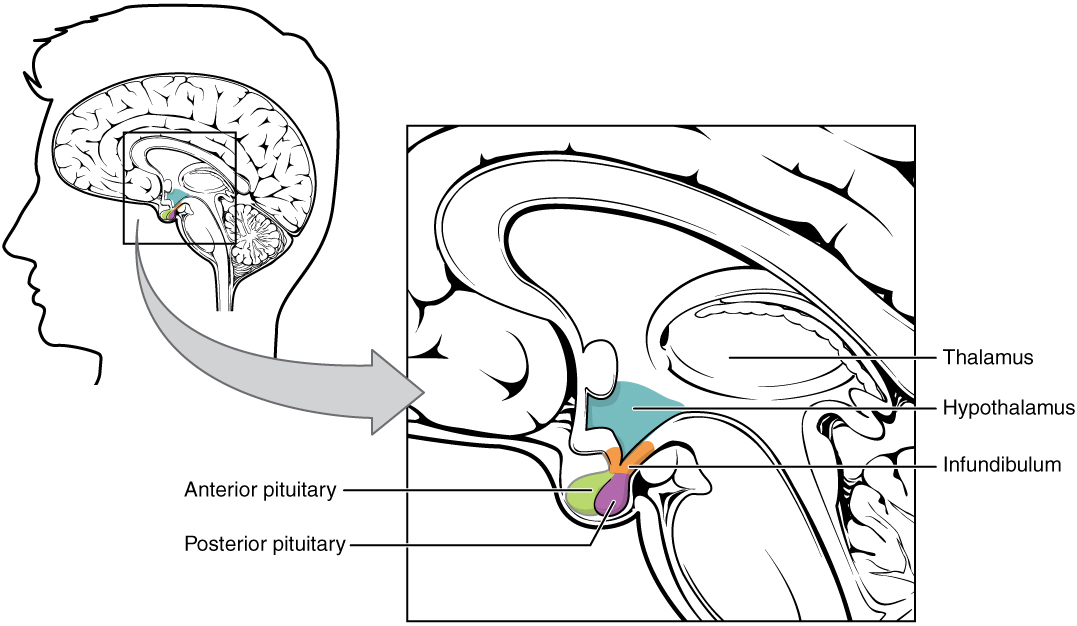
00:01 Now that we’ve looked at the basics of anterior pituitary, let us now get into the pathology. 00:06 The first topic here is going to be pituitary insufficiency. 00:11 Insufficiency, that means that we’re lacking the hormones being released from the anterior pituitary or perhaps the posterior pituitary. 00:18 Do not forget that. 00:21 Our first cause or aetiology of our pituitary insufficiency, in fact, is an adenoma. 00:26 Many a times med students and residents get adenomas and think of it as only being functioning. 00:32 Do not ever do that, especially with boards. 00:35 Even though it might be a smaller percentage of adenomas being non-functioning, if you are not paying attention to your patient or question, you get it wrong unnecessarily. 00:45 So, we have a space-occupying lesion within the pituitary that is causing decreased release or no release of a hormone at all. 00:55 We’re not quite done. 00:57 The picture that you’re seeing here, in fact, is the pituitary. 01:00 The house of your pituitary gland in fact is called the? Good, sella. 01:08 And the connection between the pituitary and the hypothalamus, as you know and we’ve talked about earlier, is the infundibulum or the stock and the circulation within it is the portal vein. 01:17 What I would like for you to do is I want you to start thinking of this adenoma growing and growing and growing. 01:27 Remember, if this is a non-functioning adenoma, a space-space occupying lesion would then knock out a respective hormone coming out of the anterior pituitary or posterior pituitary. 01:38 But, if this adenoma continuous to grow and let’s say that it compresses the stock, wow, now this is what you need to know. 01:47 Listen, if that stock has been knocked out for any reason at all, stock compression or stock severance... if you sev-severe the stock then the hormone that you’re paying attention to at that point will be prolactin. 02:06 Tell me the peptide or give me the name of the substance that-that inhibits the release of prolactin? That’s dopamine that’s coming from the brain through the hypo-hypothalamus, through the stock, to the pituitary. 02:23 So, if you compress the stock, guess what happens? You cannot deliver the dopamine to the anterior pituitary. 02:32 So, therefore, you lose the inhibition. 02:36 If you lose the inhibition of prolactin, you are then going to have excess prolactin. 02:41 However, as far as all the other hormones are concerned, it pretty much knocks them out. 02:48 Our topic right now is pituitary insufficiency. 02:50 I’ve walked you through in great detail a non-functioning pituitary adenoma. 02:57 Now growth hormone usually affected first, then FSH and LH then TSH and then ACTH last. 03:08 This is a pituitary insufficiency with an adenoma that’s non-functioning. 03:12 So, if the growth hormone has been knocked out as a child, obviously, we have dwarfism. 03:18 If it’s your gonadotropins, you’re respectively man or woman; in a man, you’d have delayed puberty whereas in a female, she’d have delayed puberty and she would have amenorrhea. 03:28 TSH should be knocked out, you tell me what kind of hypothyroidism? Primary, secondary, tertiary? Secondary, good. 03:37 See, if you did a TRH stimulation test, you would not release TSH, would you? And then ACTH… if that’s been lost, what do you call that primary, secondary or tertiary hypocorticolism? Secondary. 03:54 And that then brings you discussion of corticotrophin releasing hormone stimulation test. 04:01 Are these important points that I’m making? Absolutely because you want to know more than one biochemical test that you’re going to perform on your patient so that you can appropriately confirm your diagnosis. 04:14 Isn’t that what’s most important for your patient and for your practice and to get your question right? Other causes. 04:22 Something called pituitary apoplexy. 04:25 Do not confuse this with Sheehan. 04:27 That’s another topic, that’s pituitary infarction. 04:30 Well, pituitary apoplexy is the closest pathogenesis that I can-I can give you with this would be something like waterhouse friderichsen syndrome. 04:40 What does that mean? Remember waterhouse friderichsen syndrome that you talked about in microbiology with Neisseria species would be if there would be sudden rush of blood and haemorrhage into the adrenal cortex and you lose all functioning. 04:56 Well, the same kind of issue might be taking place up in the sella. 04:59 You might have sudden haemorrhage into the sella doing what? Causing pituitary insufficiency. 05:09 And of all the hormones, the one that you’re paying attention to quite importantly will be cortisol. 05:14 Why? Cortisol is the most important stress hormone. 05:21 Let’s continue with aetiologies of our pituitary insufficiency and this time we come to infarction. 05:27 So, this, of course, gives the age old presentation that I’m sure that you’ve been exposed to a number of times and this would be a pregnant woman who, let’s say there is a placental disease and maybe perhaps the placenta instead of attaching to the decidua, attaches to the myometrium directly. 05:52 And so, therefore, during delivery, the placenta is now being whipped away from the lining of the-of the uterus and in the process may result in pretty massive haemorrhage in a pregnant woman who is suffering from such a complication. 06:10 That massive bleeding, remember a pregnant woman’s pituitary gland is rather enlarged, hypertrophy, it has to be. 06:16 It’s a lot of responsibility that the pregnant woman is taking care of. 06:21 What that hypertrophy of course means also increased blood supply. 06:26 All of a sudden, there is massive haemorrhage during delivery. 06:30 The first organ to be knocked out or to be sacrificed unfortunately would be your pituitary gland. 06:37 Welcome to pituitary infarction causing pituitary insufficiency. 06:43 Now, how would you know that the pregnant woman is in fact suffering from Sheehan’s syndrome? Because she cannot properly breastfeed her child all because there is no prolactin. 06:59 However, what’s the hormone that you want to replenish to make sure the survival of your patient? Good, cortisol. 07:08 Remember, infarction, the entire pituitary gland is probably compromised. 07:15 What else might cause pituitary insufficiency? Maybe lymphocytic, what’s known as hypophysitis. 07:23 Usually found in postpartum women. 07:24 So, literally, there’s going to be lymphocytic infiltration causing destruction. 07:31 Unfortunately, there is still radiation and can’t say that it’s not without side effects and serious issues including the fact that radiation may cause damage to the pituitary gland or for that matter any organ, huh? Or you take a look at the sella and there’s nothing home. 07:52 You see the house? Well, there’s no one home. 07:55 Welcome to empty sella… pituitary insufficiency. 08:00 Or there might be infectious or granulomatous or even cancers that may cause destruction to the pituitary. 08:09 A list of important differentials of pituitary insufficiency. 08:14 Let’s walk through each one of these hormones and what is the result of lack of that hormone because of hypopituitarism or pituitary insufficiency? Say that three times fast, haha! So, say there is no growth hormone, your cartoon here on your right is showing you a normal male at a normal height or you find this child who doesn’t have growth hormone resulting in dwarfism. 08:50 IQ normal, this is not a cretin, okay? This isn’t a patient with lead poisoning, okay? There’s also short stature children, but in dwarfism, you have a dwarf... nor is your patient here achondroplasia, right? Achondroplasia, you look like this, short limbs, but the head is perfectly normal, the trunk is normal because the flat bones are normal. 09:20 Do not get achondroplasia, which is a very common cause of short stature and dwarfism, and make sure you know the characteristics. 09:30 IQ here perfectly normal and it’s proportional stunted growth. 09:37 Next, growth hormone is a stress hormone. 09:42 So, now, let’s group together biochemically the stress hormones that you’ve seen together. 09:48 You always put together cortisone, glucagon that takes care of two. 09:51 You are going to put in there in the mix epinephrine and your growth hormone. 09:58 What is the-What is this stress hormone always going to do? It’s always going to find a way to increase glucose in your circulation, isn’t it? Yes, it is. 10:06 It’s always going to promote glucose and plasma. 10:12 So, if you don’t have growth hormone, you can expect what type of glucose levels in an adult? Hypoglycemia in adults. 10:22 Let’s talk about gonadotropins. 10:26 If the gonadotropins have been compromised due to hypopituitarism or pituitary insufficiency, then there’s going to be, as we discussed, early, delayed, retarded sexual maturation in children. 10:38 If it’s an adult and if it’s a male, we talked about decreased libido, impotence, muscle loss and facial hair is not present or is not in abundance. 10:53 If it’s a female and she doesn’t have a gonadotropin, she doesn’t have her LH and FSH. 10:58 So, therefore, she will not have an LH surge, she will not have ovulation, she doesn’t even have the FSH to have the proliferative phase. 11:07 So, guaranteed your female is amenorrheic. 11:13 If there’s pituitary insufficiency and TSH is not present, this is secondary hypothyroidism. 11:21 Your patient obviously is going to feel tired, fatigue, slow down, a little bit of food and increased weight and maybe constipated. 11:32 You give TRH, obviously here, you are not going to release TSH from the anterior pituitary. 11:38 If ACTH isn’t present, this is called what? Secondary, secondary hypocorticolism, not primary. 11:46 If you give CRH, you are not going to find stimulation and release of ACTH. 11:51 Here, you will obviously find decreased levels of cortisone, but you will not find hypopigmentation because this is not Addison’s. 12:01 Is that clear? What’s Addison’s? Primary hypocorticolism. 12:07 If you’re confused with this, it’s okay. 12:08 What this is saying here is the fact that compared with C/W stands for compared with Addison’s, secondary hypocorticolism will not have hypopigmentation and that is a huge point. 12:27 And if you do not have cortisol, welcome to RIP.
About the Lecture
The lecture Hypopituitarism by Carlo Raj, MD is from the course Pituitary Gland Disorders.
Included Quiz Questions
Because of compression from a pituitary adenoma, which pituitary hormone is first affected?
- Growth hormone (GH)
- Follicle-stimulating hormone (FSH)
- Luteinizing hormone (LH)
- Adrenocorticotropic hormone (ACTH)
- Thyroid-stimulating hormone (TSH)
Which hormone will increase as a result of a nonfunctioning pituitary adenoma causing compression of the infundibulum?
- Prolactin
- Growth hormone (GH)
- Thyroid-stimulating hormone (TSH)
- Gonadotropin-releasing hormone (GnRH)
- Adrenocorticotropic hormone (ACTH)
Which cause of pituitary insufficiency most commonly occurs late during pregnancy or postpartum?
- Pituitary adenoma
- Hemorrhagic pituitary apoplexy
- Ischemic pituitary apoplexy
- Lymphocytic hypophysitis
- Trauma
Which hormone abnormality is most likely to cause hypoglycemia in adults?
- Growth hormone deficiency
- Gonadotropin-releasing hormone deficiency
- Insulin deficiency
- Increased thyroid-stimulating hormone
- Increased adrenocorticotropic hormone
An adult male presents with impotence, muscle atrophy, and loss of facial hair. Which hormone abnormality is most likely?
- Follicle-stimulating hormone deficiency
- Growth hormone excess
- Estrogen deficiency
- Increased serum adrenocorticotropic hormone
- Thyroid-stimulating hormone excess
Author of lecture Hypopituitarism

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
understandable and makes sense, teaches more than required for the boards.
