Playlist
Show Playlist
Hide Playlist
Cluster Headache

-
Slides Headache AcuteCare.pdf
-
Download Lecture Overview
00:01 So, do you remember the worst headache of your life? Or if you’ve ever had a headache that really just knocked you out of commission? I can think of two times, both when I should have been in happy, fun places where I had a headache and I just could not move because the pain was so bad. 00:17 And one of them, I actually thought, oh my goodness, is this the big one, am I having an aneurysm? But it resolved once I just took a little bit of rest. 00:24 And so, luckily, I don't have a headache disorder, but a lot of people do. 00:28 And therefore, it's really important to consider both, again, for your exam and for your clinical practice. 00:33 So, we’ll be going over the diagnosis and management of headache today. 00:39 So, common cause of the headache, most common by far is tension headache. 00:43 Migraine, much less common, but still affects millions of adults. 00:47 Cluster headache, pretty rare, but we’ll discuss it briefly as well. 00:51 Just to understand, so overall in the United States, about half of the adults have one of these types of headache disorders. 00:59 So, a tension-type headache, the classic is mild to moderate pressure that's over the head. 01:05 It kind of forms a helmet-like distribution, kind of starting in the temples, but it can go back. 01:10 It can certainly also involve the neck as well, the posterior neck, and there you can actually feel the tension sometimes. 01:17 Compared with migraine, it’s less aggravated by physical activity, but if you have a tension headache and you go out and do something particularly active with a lot of lifting, you can expect that your headache is going to get worse. 01:30 That said, it’s rare in tension-type headache alone to have nausea, vomiting with either photo or phonophobia. 01:37 And a lot of times, it is related to stress, anxiety, other mood disorders and that's – those are the things that are typical for tension-type headache. 01:46 Migraine headache, you can use the acronym POUND to get an idea of its etiology and its diagnosis. 01:55 So, first of all, the pain has a pulsatile quality to it in its classic form. 01:59 It can be on for 44 to 72 hours. 02:03 It's often unilateral. 02:05 It’s associated frequently with nausea and vomiting and the photo and photophobia. 02:10 And then finally, it's associated with disability in many cases because these can be severe headaches. 02:16 Whereas cluster headache, we talked about it, it's more rare. 02:19 It's also more severe. 02:21 This is a headache that’s more common among males versus females. 02:25 It is associated with a family history, but the family history isn’t always present. 02:29 It’s severe headaches – when the cluster comes on and it can be over a space of a few days or a week where the headaches are very frequent, these are usually severe and debilitating, often associated with autonomic dysfunction with tearing and rhinorrhea. 02:46 It’s usually over the face, temporal or periorbital pain. 02:49 And as I said, sometimes, there is a family history, but oftentimes there is not and these arise de novo. 02:56 There are patients who have cluster headaches every 5 to 6 months. 03:02 There's patients who have cluster headaches once in their lifetime and it never returns again. 03:07 It’s a variable course. 03:10 So, what you want to know when you see a patient with headache, is headache dangerous? Am I worried about this headache? Could this be a mass, aneurysm, tumor, some of these very bad things, meningitis, encephalitis? If the headache is a little bit recurrent and not presenting in the emergency department, say, with fever and stiff neck, which would be consistent with meningitis, for most patients who to come into a clinical setting, these are some criteria that make you think the headache may be less dangerous. 03:39 Age over 30, but under 75, less dangerous. 03:44 Have they had this headache before? If it's characteristic and consistent with previous headaches, that's reassuring. 03:51 There's no change in the headache pattern, it’s not growing worse, it’s not associated with new symptoms, the pain isn’t moving around in their head. 03:58 High-risk conditions, so things like HIV for chronic infections, previous intracranial aneurysms is the number one risk factor for another aneurysm. 04:10 Another risk factor for aneurysm, rare conditions such as Marfan syndrome. 04:15 And then, you’re going to do a physical examination. 04:18 Everybody with a headache – and I see many patients with headache, they deserve a neurological exam. 04:23 Doesn’t mean you have to repeat it every time they come in because they are coming in for their hypertension, their diabetes, and you also are monitoring your headache, you don’t have to do a neurological exam every time, but certainly you’re going to do a complete neurological exam, at least on that incipient visit when they have their headache. 04:40 And any abnormal finding, think about getting imaging.
About the Lecture
The lecture Cluster Headache by Charles Vega, MD is from the course Acute Care. It contains the following chapters:
- Headache
- Cluster Headache
Included Quiz Questions
A 38-year-old woman presents with recurrent headaches over the past 3 months following her promotion at work. On average, headaches occur 1 week a month. They are usually mild, bilateral, tightening, and non-pulsating. She has no nausea or other associated symptoms. Which of the following is the most likely diagnosis?
- Tension-type headache
- Migraine
- Cluster headache
- Hypothyroidism
- Berry aneurysm
Which of the following best describes cluster headache?
- Severe unilateral orbital or temporal pain accompanied by ipsilateral autonomic phenomena
- Severe unilateral orbital or temporal pain accompanied by contralateral autonomic phenomena
- Severe bilateral orbital or temporal pain accompanied by bilateral autonomic phenomena
- Severe bilateral orbital or temporal pain without autonomic phenomena
- Severe unilateral orbital or temporal pain without autonomic phenomena
Which of the following descriptions of nontraumatic headache is most concerning?
- New and severe headache
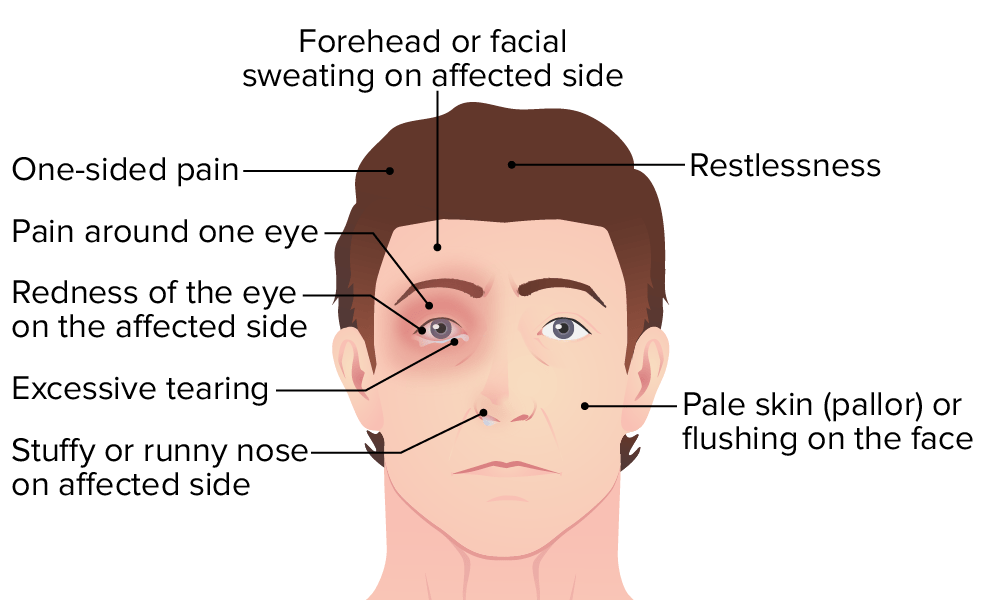
- Unilateral pulsating headache with nausea and photophobia
- Moderate, bilateral, tightening, and non-pulsating
- Unilateral throbbing headache with nausea and phonophobia
- Bilateral, tightening, non-pulsating, and not affected by movement
Author of lecture Cluster Headache

Charles Vega, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
