Playlist
Show Playlist
Hide Playlist
Proximal Convoluted Tubule (PCT): Proximal Nephron

-
Slides PCT Pathophysiology RenalPathology.pdf
-
Download Lecture Overview
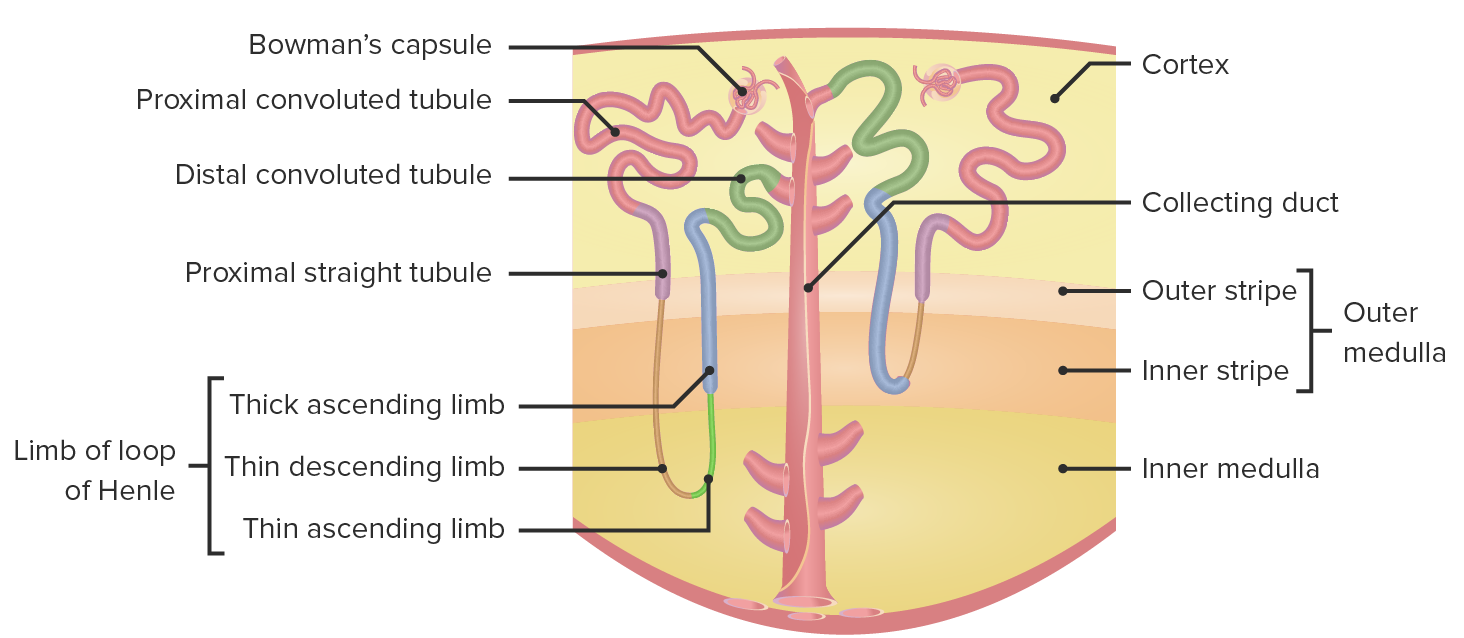
00:01 Up until now we have looked at overview of the nephron and we have introduced the different parts of the nephron and I have gone through an overview. And at some point if you got a little confused or perhaps even tripped up with some of the information that I have given you, not to worry, reinforcement. So here we will walk into and dive into further detail of each segment of the nephron and go through all the relevant information so that you can get your questions on any aspect of medicine on the nephron absolutely correct. 00:36 So let us take a look at the PCT in that respect. Once again, to review, take a look at this. 00:43 Obviously, I am not going to spend time going through each one in details, but I will go through the details of what I referred to. For example, the carbonic anhydrase and its inhibition and what that means to you? Stop here for one second and what does that mean to you if you inhibit that enzyme? You are getting rid of your bicarb. Why might you want to do that? Do you remember our discussion on high altitude? How fast are you breathing? Very quickly. Blowing off the carbon dioxide so maybe perhaps you might want to on purpose, help your patient by inhibiting the carbonic anhydrase so that patient can then compensate by getting rid of that bicarb in the kidney. At this point, you should be able to figure out what the figure looks like in its organization pattern? I have established that over and over again in previous discussions. For example, on the left is your urine, in the middle is your cell and on the right is your interstitium, moving towards your blood. We have also very much established our definitions as to what it means to be reabsorbing versus what it means to be secreting? Now with the PCT, further detail. And the early portion is where we are, and we will go ahead and call this a brush border. What does that mean to you? Now once again you know me well enough where I draw parallels to many organ systems, from head to toe. Here well in the proximal convoluted tubule when you say brush border, you must be referring to the luminal membrane, the apical membrane. If you are referring to the brush border membrane, more importantly in the duodenum, really think about where you would be if it is a duodenum. So if it is a duodenum especially second part where there is quite a bit of guess what? Reabsorption. Guess what that apical membrane is known as? Brush border. Is that clear? So simple definitions in which you can apply to different organ systems. Let us continue. 02:39 What kind of things that you are going to absorb in the proximal convoluted tubule? We have spent a heck of lot of time with reabsorbing bicarb, reabsorbing glucose especially with the graph where we talked about the normal plasma glucose, talked about threshold, transport maximum, talked about reabsorptions, splay, and so forth. And if you finished that discussion, then I would recommend that you go back and take a look at that graph on glucose transport in great detail and then come back here and then just take a look at as to where it gets reabsorbed. It has to be a secondary type of transport with sodium- potassium pump at the basolateral membrane. Let us continue please. 03:17 Isotonic. Now this is important. In a little bit, I am going to show another graph. And this graph, at some point right now, maybe you might be feeling a little overwhelmed, maybe perhaps even frustrated, or that are yet you are feeling fantastic about these graphs because you saw them in medical school. And maybe you looked at it, glanced at it, maybe you even memorized it, but you didn't truly understand that until now and so therefore you feel enlightened. You feel confident. You feel really you can tackle this. And there is another graph that's upcoming in which we will take a look at transport especially in the PCT. Now before we get there though you need to understand as to how you might be taking up some of the substances. 04:05 It is important. I have just left the Bowman space. I have entered the PCT. That is where we are. So now what are you going to reabsorb? Many electrolytes. How much of sodium? 2/3, 66 percent approximately, same thing. Is that sodium that you only reabsorbing? I want you to think PCT, what's my next segment of the nephron? Tell me that, I hear you say descending loop of Henle. The descending limb of the loop of Henle. What is going on there? You are reabsorbing water. So if you start reabsorbing the water, what kind of urine are you producing? Hypertonic by the time you get to the loop of Henle. Are we clear? Good. So in the PCT though, so further proximal, you are going to reabsorb your sodium along with water in what kind of fashion? Isotonic. What does isotonic mean to you? Approximately how much? Keep it simple. 300 mOsm. So that term isotonic becomes very crucial for you to recognise here in the PCT. Now what else is the PCT known for? It is all important, ammonia. What is ammonia? NH3. What if you add another hydrogen? Why would you add another hydrogen? To buffer. When was the last time you have heard of ammonia in medicine as far as your level of education what you need to know? A few times. Number 1, you have heard of ammonia in terms of microbiology. Really? Yeah, in the kidney actually. So at some point when we talk about nephrolithiasis or renal stone, we will talk about a particular stone that is huge. It is called a staghorn stone or you call it a struvite. What is it made up of? M, magnesium. 06:13 A, ammonia. P, phosphate. So you tell me what kind of organisms would be involved with the stone that is made up of magnesium, ammonia, phosphate? Alkaline organism, give me one. 06:30 Proteus mirabilis. So you have heard of ammonia before. You know that it is already alkaline in nature. These are things that you have it memorized, which you have given a clinical correlations and in a disease such as that, well then you know that it is already alkaline. 06:46 Where else have you heard of ammonia? What am I doing here? I like you too. I am waving, but I cannot help this. I am doing resting tremors. What is this called? Asterixis. Tell me what organ has been involved, resting flapping tremors like this. It means my liver alright. Liver is responsible for proper metabolizing of the ammonia. What if you have cirrhosis? Then ammonia starts accumulating in the head. It is called hepatic encephalopathy, and what's your sign? Asterixis. So you have heard of ammonia in a couple of places that are very important. Let us talk about ammonia here. Where am I? PCT. 07:27 And if it is alkaline, what does that mean to you? Its responsibility here. In the PCT, where it is generated. See that right there, generated here. That is important. Not recycled, but generated in the PCT. At some point, down in the DCT, guess what it picks up? The hydrogen. 07:49 When it does, then you call it ammonium. So when you add a H, you add a M, you take off that H, you have ammonia NH3. NH4. Let us move on. 08:03 Still in the PCT and at this point let us talk about PTH. Isn't it interesting as to how in the PCT, we have so many different things going on that are so clinically relevant. 08:15 Spend a little bit time, make sure that you understand this well. Now PTH, tell me two things that it does in the kidney. In general, in the kidney, reabsorption of calcium, is that taking place here? No. Where am I? PCT. What is the other job of PTH? It is to flush out the phosphate. In other words, it inhibit the reabsorption of phosphate. Isn't that the same thing in terms of the consequence? Yes. So you are flushing out the phosphate, inhibiting the reabsorption of phosphate where? This ladies in gentleman is in the PCT. I did mention this prior, but now we are now actually stating it here. You increase phosphate excretion. So this bullet point, say that your pathology in which you increase your PTH, either primary or secondary. Let us talk more about primary. I will tell you why when I am using secondary later. We are only going to talk about primary. Primary hyperparathyroidism. Where is your adenoma? In the parathyroids where you producing too much of PTH. Where are you going? Down to the kidney. Here specific in the PCT, what are you going to do? You are going to excessively inhibit the reabsorption of phosphate. Tell me about your phosphate levels in your urine. Hyperphosphaturia, hypophosphatemia. You see what I just did there? I have increased the phosphate in my urine and that is exactly how medicine works it. It is hyperphosphaturia, hypophosphatemia. The more that you get rid of your phosphate into the urine, the less that you have it in your plasma. Are we clear? Next, where more in the PCT? Brings us way back to angiotensin II. Now before you just memorize this which you know that I don't want you to do. When you do want to release angiotensin II? Anything that causes decrease perfusion of fluid or plasma to the kidney. Right? Give yourself two major examples. One would be renal artery stenosis. Are you seeing it? And the other one is congestive heart failure. Two totally different reasons, but ultimately what happens? Decreased perfusion to the kidney. So therefore what are you going to release? Renin and here comes my angiotensin II. And angiotensin II, too many other different places that it works, universal vasoconstrictor, so it works on major systemic arteries to cause vasoconstriction, increasing thus afterload. Angiotensin II works on adrenal cortex. It works specifically in the glomerular, to do what? Release aldosterone. Angiotensin II also works in the efferent arteriole, preferentially efferent, to constrict it so that you can restore GFR. Angiotensin II works here in the proximal convoluted tubule so that you can reestablish that lost blood pressure. So it reabsorbs sodium and exchange for hydrogen. Are we clear? Permitting contraction alkalosis. Remember, the more that you reabsorb sodium, I want to take a look at that on that apical membrane, right there, on the luminal side, not the sodium- glucose symport. The sodium-hydrogen antiport is what I want you to pay attention here because that is where angiotensin II is going to work. Are we clear? So what do you think angiotensin II is going to do? Why you are releasing this? Decrease blood pressure. 11:37 So you are going to reabsorb sodium and exchange for what? Hydrogen. You get rid of your hydrogen, what happens to your pH? Increased. Welcome to contraction alkalosis. 11:49 Now, this table we are going to spend time here. And by the time we are done, you will
About the Lecture
The lecture Proximal Convoluted Tubule (PCT): Proximal Nephron by Carlo Raj, MD is from the course Diseases of the Nephron.
Included Quiz Questions
Which of the following statements about sodium reabsorption is TRUE?
- It primarily occurs in the proximal convoluted tubule.
- It is primarily reabsorbed in the form of sodium hydroxide.
- It is responsible for paracellular transport of other cations.
- Reabsorption is inhibited in the proximal convoluted tubule by parathyroid hormone.
- It is exchanged for K⁺ in response to aldosterone stimulation in the proximal convoluted tubule.
Which of the following findings is common in severe liver disease as a result of the accumulation of ammonia in the body?
- Flapping tremor
- Gynecomastia
- Easy bruising
- Jaundice
- Caput medusae
Which of the following statements about ammonia is INCORRECT?
- All options are correct.
- It has alkaline properties.
- It is metabolized in the liver.
- It converts to ammonium in the distal convoluted tubule.
- The formula is NH₃.
Which of the following laboratory changes is most likely in primary hyperparathyroidism?
- Hyperphosphaturia
- Hyperkalemia
- Hyperphosphatemia
- Hypocalcemia
- Hypophosphaturia
Which of the following changes may result from the action of angiotensin II?
- Decreased urine pH
- Vasodilation of the afferent arteriole
- Increased urine sodium concentration
- Vasodilation of the efferent arteriole
- Increased calcium reabsorption
Author of lecture Proximal Convoluted Tubule (PCT): Proximal Nephron

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Dr. Raj is breaking this down and is the reason I will likely resub my lecturio. Clear, concise, and engaging.
