Playlist
Show Playlist
Hide Playlist
Pituitary Sellar Masses

-
Slides AnteriorPituirary EndocrinePathology.pdf
-
Download Lecture Overview
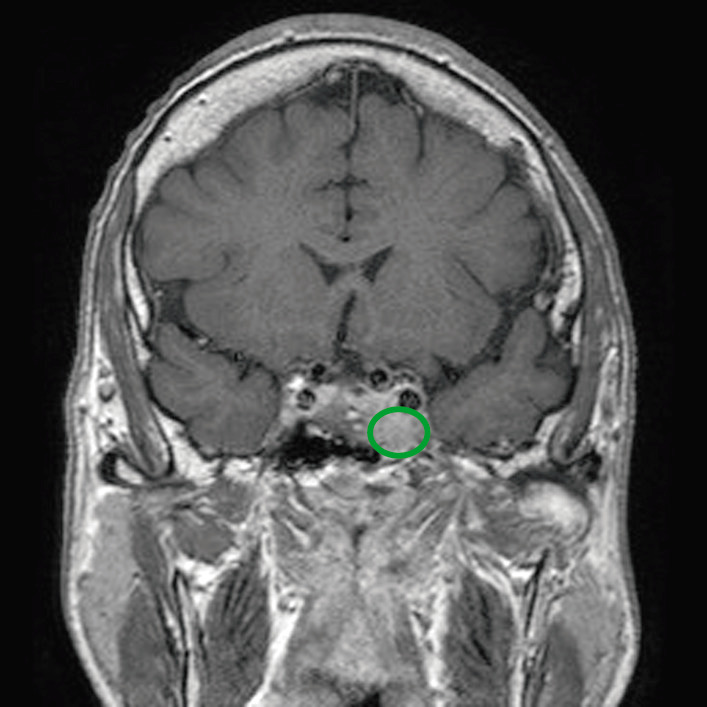
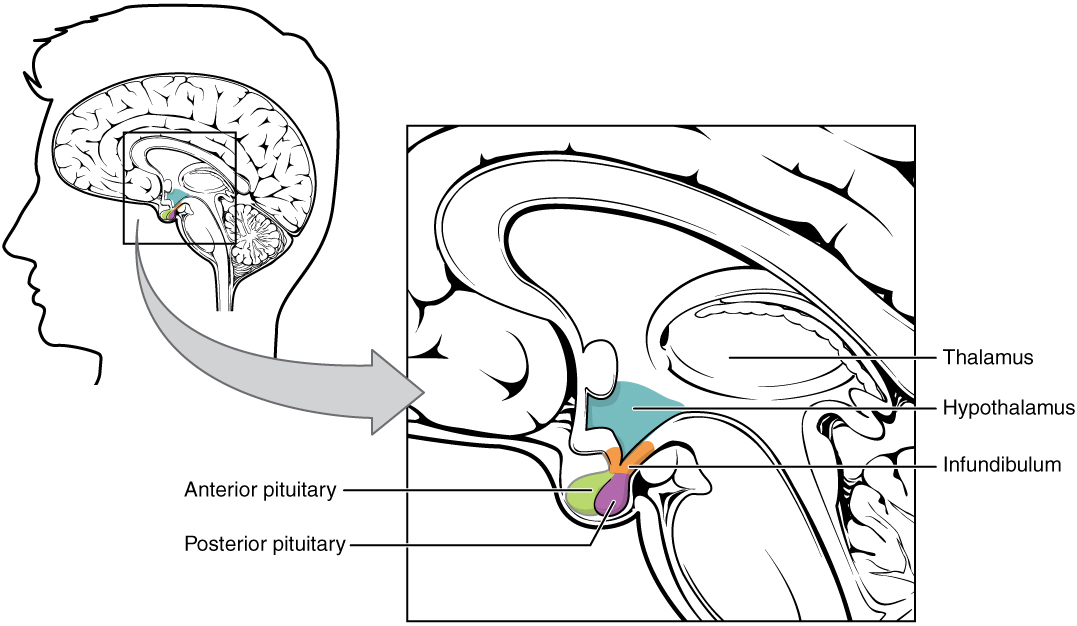
00:02 Let’s talk about sellar masses. 00:04 So, whenever you have a mass within the sella, things that you’re always looking for symptomatically are your neurologic issues, especially headaches and visual impairment. 00:15 We talked about this just now. 00:19 Often times these sellar masses are incidental on-on MRIs and may often times be known as incidentalomas microadenomas in normal population. 00:31 So, this might have been there the whole time, an incidentaloma. 00:38 Hormonal abnormalities may also occur, obviously if there are sellar masses. 00:42 Here, I want to show you a second messenger system that you want to be clear about. 00:51 We have GTP beta and gamma. 00:55 This, as you remember from biochemistry, is inactive G-protein. 01:01 What must you have so that you can have proper activation of your enzyme? You have to make sure that you hold on to your alpha, right? So, you then become an alpha, active G-protein and when you do so, you might then stimulate an enzyme called adenylyl cyclase. 01:23 And that adenylyl cyclase will convert your ATP into cyclic AMP. 01:27 And if you remember correctly that at some point in time, you will then remove a phosphate so that you can inactivate it and then turn into your GDP. 01:38 Now, with all that said, let’s get into our topic of what’s known as MEN1, multiple-multiple endocrine neoplasia type 1. 01:50 Your first thing that you want to do is, well, identify your patient. 01:55 Usually, family history is taking place and when you deal with MEN1, it is a triade. 02:02 The triade here is going to be called pan-para-pit, as we’ll talk about later. 02:07 You’ll have pancreatic tumour, you’ll have a hyperparathyroid, hence the hypercalcemia and the kidney stone. 02:15 So, some of the things that you want to pay attention to right off the bat with MEN1 is family history and whether or not kidney stones of calcium type. 02:25 In addition is pancreas and then when you say pituitary, you’ll have prolactin levels being elevated. 02:33 In your female, may result in galactorrhea and she’s going to be amenorrheic. 02:40 The reason that we went through the G-protein in great detail is the following. 02:44 Understand that these adenomas and these tumours that you’re going to find in MEN1 often tend to be constitutive activation of your Gs... 02:58 Gs and hopefully, what you remember is that of all of the hormones that you’re going to release pathologically from a functioning adenoma… Remember, up until now, our discussion earlier was... has been a dysfunctional or a non-functional adenoma. 03:19 In non-functioning adenoma, the first hormone to be knocked out is growth hormone hence, we walked through dwarfism. 03:28 Whereas if it’s a functioning adenoma, the number one hormone to come out would be your prolactin. 03:35 So, here, when we talk about 40% of somatotroph adenomas, that’s exactly right because the prolactin or prolactin is a somatotropin, isn’t it? So, therefore, you can expect there not only to be prolactin, but at times maybe excess growth hormone. 03:55 What’s my problem? Biochemically and genetically, there might be an issue with my Gs-protein. 04:01 What does Gs mean to you? In order for you to be active, you have to have the alpha sub-unit. 04:11 Pituitary transforming genes, something called PTTG. 04:16 Pituitary transforming genes - associated and also fibroblast growth factor receptor-4. 04:21 I would make sure that to memorize some of these growth factors here and some of these genes and something that you already know from biochemistry with these G-proteins so that you have constitutive activation. 04:34 Let’s do classification of our pituitary tumours. 04:40 If it’s less than 1, it’s microadenoma. 04:44 If it’s greater than 1, we call it a macroadenoma. 04:48 Gonadotrophs adenomas usually present clinically as a non-functioning sellar mass. 04:54 That’s interesting, isn’t it? Thyrotroph adenomas may present clinically as non-functioning sellar mass that secrete only alpha or TSHbeta sub-unit and may cause hyperthyroidism due to increased secretion of intact TSH. 05:11 So, what we’ll do here as we’re going through our topics of adenomas is, well, specifically what kind of hormone are you producing from your adenoma? 40%, do not forget, would be what kind? Somatotrophs, right? So, that would include both prolactin and growth hormone. 05:30 Now, we have gonadotrophs, thyrotrophs, corticotrophs, lactotrophs and somatotrophs. 05:39 The combination adenomas are well recognized to clinical syndrome of both prolactin and growth hormone. 05:46 Do not forget that. 05:48 And naturally, your emphasis should be when you talk about functioning adenomas, the bottom two statements here. 05:55 In the meantime though, when you have a functioning adenoma, always pay attention to your patient in your stem and is your patient in fact suffering from Cushing’s disease. 06:05 You’ll notice Cushing’s disease and not Cushing’s syndrome. 06:10 Cushing’s disease is specifically increased cortisol due to ACTH coming from the anterior pituitary. 06:22 We’ll talk more about this when the time is right, but at this point, it is imperative that you specifically know the difference between Cushing’s disease and Cushing’s syndrome, as we shall see, or otherwise you will miss a question unnecessarily. 06:39 What we’re seeing here would be a pituitary adenoma and with an MRI, you’ll find enlargement of the pituitary compressing the optic chiasm resulting in visual disturbances. 06:59 The topic prolactin, just to make sure we’re clear. 07:04 We saw this in the very beginning where I walked you through many types of releasing hormones above the dash line representing the hypothalamus and the various anterior pituitary hormones below the line. 07:18 Our focus… I also had you pay attention to dopamine, normally inhibiting the prolactin and, as you can see here on the side branch, thyrotropic releasing hormone stimulating prolactin release. 07:35 One step further, I also gave an example where you can have a non-functioning adenoma in the sella which is then compressing the stock, diminishing or delaying the delivery of dopamine to your prolactin, thus increasing release of prolactin. 07:55 Do not ever forget that. 07:59 Prolactin, what does it do? Lactation in women. 08:05 Now, is this the hormone when the infant is suckling on the mother’s nipple? Is this the hormone that’s responsible for ejection of milk? No. 08:18 This, however, is the hormone that’s responsible for synthesis of milk. 08:24 Now, don’t be so black and white where you’re thinking, “Well, if I have a prolactinoma, if I have a hyperprolactinemia, if it’s not physiologically responsible for ejection…” I don’t want you to think that you wouldn’t have galactorrhea. 08:40 Listen, if you have too much prolactin for whatever reason, either prolactinoma or functioning adenoma in the anterior pituitary, maybe it’s due to antipsychotics, maybe it’s lesions in the stalk, maybe compression of the stalk, whatever it may be, that hyperprolactinemia is going to have so much milk synthesis and which, at some point, of course, you’ll have galactorrhea. 09:07 Regulation, we talked about TRH stimulating prolactin. 09:13 And so, therefore, it is extremely high in primary hypothyroidism. 09:20 Dopamine inhibits prolactin release.
About the Lecture
The lecture Pituitary Sellar Masses by Carlo Raj, MD is from the course Pituitary Gland Disorders.
Included Quiz Questions
Which pathology is the most common cause of visual impairment in patients with sellar masses?
- Compression of the optic chiasm
- Compression of the visual cortex
- Increased intracranial pressure
- Decreased intraocular pressure
- Cavernous sinus thrombosis
What is the triad of neoplasia that characterizes multiple endocrine neoplasia type 1 (MEN1)?
- Neoplasia affects the parathyroid gland, pancreatic endocrine tissue, and anterior pituitary gland
- Neoplasia affects the thyroid gland, pancreatic endocrine tissue, and anterior pituitary gland
- Neoplasia affects the thyroid gland, pancreatic exocrine tissue, and anterior pituitary gland
- Neoplasia affects the thyroid gland, pancreatic exocrine tissue, and posterior pituitary gland
- Neoplasia affects the parathyroid gland, pancreatic exocrine tissue, and posterior pituitary gland
What is NOT associated with a pituitary adenoma?
- Lymphocytic hypophysitis
- Prolactinoma
- Multiple endocrine neoplasia type 1
- Pituitary apoplexy
- Bitemporal hemianopia
Which mechanism leads to increased prolactin secretion following compression of the pituitary infundibulum?
- Blocked delivery of dopamine
- Overproduction of dopamine
- Increased availability of hypothalamic releasing hormones
- Blocked delivery of hypothalamic releasing hormones
- The positive hypothalamic-pituitary feedback loop
Author of lecture Pituitary Sellar Masses

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
