Playlist
Show Playlist
Hide Playlist
Tracheal Development

-
Slides 06-36 Development of the large airways.pdf
-
Download Lecture Overview
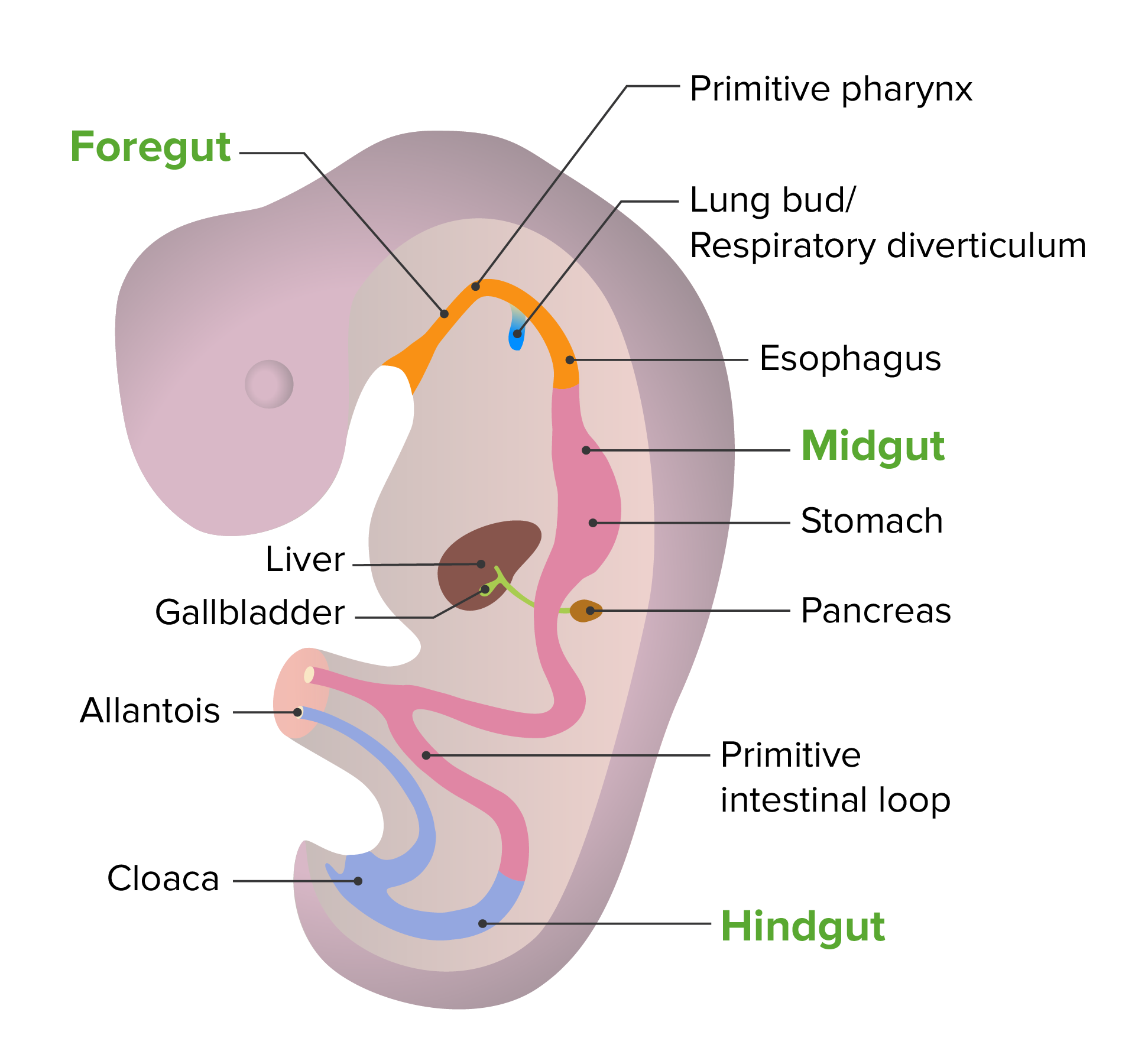
00:01 We will now discuss the development of the large airways, the larynx, the trachea, and the bronchi as they develop off of the gut tube. 00:08 The gut tube and specifically, the foregut region of the gut tube have a small diverticulum develop off of it called the respiratory diverticulum. 00:17 Also sometimes called the lung bud. 00:19 This is gonna grow into the surrounding mesenchyme and induce formation of the lungs and the rest of the airway. 00:26 Now, what would make a lot of sense would be for this respiratory diverticulum to extend off the foregut and just keep growing inferiorly, making the larynx, making the trachea, and then, splitting into the bronchi. 00:39 But that's not actually what happens. 00:41 What happens is the respiratory diverticulum comes off but remains relatively close and partially in contact with the esophagus as it does so. 00:51 The reason they get separated is because two ridges of mesenchyme are going to grow inward and these tracheoesophageal ridges grow closer and closer together on the right and the left until they fuse creating a tracheoesophageal septum. 01:08 So that wall between the trachea and the esophagus has hopefully, completely separated those past the opening of the larynx. 01:17 But they do remain connected at the laryngeal inlet. 01:20 That place where the air goes down the airway and the food can continue down the esophagus. 01:26 And as development proceeds, those two tubes further separate until there are two completely distinct but parallel structures. 01:34 Now, things that can go wrong in this process include incomplete separation of the esophagus and the trachea, and this can commonly result in a laryngeal cleft. 01:44 This is basically a small slit that's connecting the esophagus to the trachea and that's obviously not gonna be a great thing because you don't want food in your airway or air going into your esophagus and stomach. 01:57 So what's going to happen most commonly in this case is that patients will feed and as infants, they'll be feeding on milk or formula and a bit of that formula or milk will move into their airway and they'll start aspirating it, coughing, to try to expel it. 02:12 Other things that are a little bit more severe that can go wrong in this process include a variety of tracheoesophageal fistulas. 02:20 Inappropriate connections between tubes that shouldn't be there. 02:25 Now, the most common version of this is going to be the one that we see up on the screen. 02:30 It's gonna be presenting with a blind pouch at the end of the esophagus. 02:35 So esophageal stenosis and then, the distal esophagus connects to the trachea. 02:41 So in this case, an infant that's born with this is going to attempt to feed but the food has nowhere to go once it reaches that bottom of the esophageal sac, that little stenotic region. 02:52 And so, it will back up and the patient will vomit back the formula or milk and it won't have any bile in it because the biliary system is much further down. 03:02 So immediate nonbilious emesis is a hallmark of this condition. 03:06 Another thing that frequently happens is that there will be air in the stomach and if you take an x-ray, you might see some bubbles of air in the stomach. 03:13 Now, that's not super uncommon on its own but it will be very pronounced in these patients because they've got a direct connection from their airway to the stomach and no way for food to get there. 03:26 Less common but somewhat, more dramatic, are gonna be what are called H type malformations of the tracheoesophageal fistula. 03:34 In this case, we have a separate esophagus, separate trachea, but a tube connecting them forming a capital H. 03:42 In this case, we are gonna have frequent aspiration of food as well as air travelling into the digestive system and any variation on this sort of theme that you can imagine can probably occur. 03:54 The other ones are not as common as the proximal blind sac of the esophagus and distal fistula between the airway and the distal esophagus. 04:03 But any of these other variants can occur and are gonna commonly present with aspiration if there's any connection of the esophagus to the airway. 04:13 These are gonna need to be surgically corrected and fortunately, you can lengthen some of these structures and anneal the esophagus to the blind pouch and separate it from the airway entirely.
About the Lecture
The lecture Tracheal Development by Peter Ward, PhD is from the course Development of Thoracic Region and Vasculature.
Included Quiz Questions
The laryngotracheal tube and the esophagus separates from each other as development progresses but remains connected at what area?
- Laryngeal inlet
- Tracheoesophageal septum
- Groove
- Tracheoesophageal ridges
- Choanae
What is the most common type of tracheoesophageal fistula?
- Esophageal atresia with distal tracheoesophageal fistula
- Isolated esophageal atresia without tracheoesophageal fistula
- Isolated tracheoesophageal fistula
- Esophageal atresia with proximal tracheoesophageal fistula
- Esophageal atresia with proximal and distal tracheoesophageal fistula
Author of lecture Tracheal Development

Peter Ward, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
