Playlist
Show Playlist
Hide Playlist
Acute Respiratory Distress Syndrome (ARDS): Pathogenesis

-
Slides ARDS RespiratoryPathology.pdf
-
Download Lecture Overview
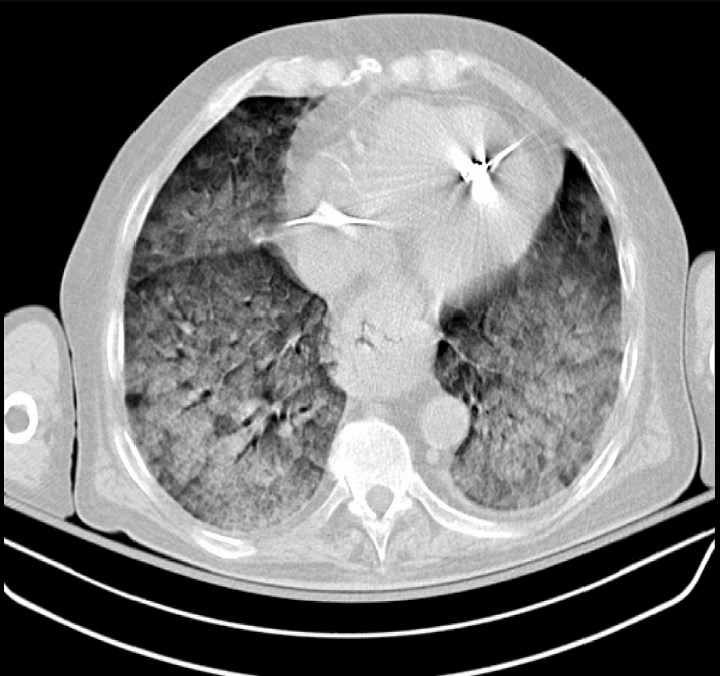
00:02 On this topic of acute respiratory distress syndrome, students have a hard time figuring out what exactly caused the collapse of the alveoli. 00:11 Let’s begin. What is ARDS? It used to be, once upon a time, may be called Adult Respiratory Distress Syndrome, but you can no longer do that because it’s very possible that you might find the causes that we will see here commonly for ARDS including sepsis that might also take place in children. A clinical manifestation of a diffuse alveolar damage. 00:34 The operative word here is alveoli in which it gets damaged. Then what happens? It disappears. It collapses. Results in atelectasis. What does that mean to you in terms of pathophysiology? Is this a dead space or is this a shunt? This is going to be a pulmonary shunt. You will see as to how that become important for us as we move further into our lecture. Diffuse alveolar damage is the final common pathway for a variety of insults to the lung. So, therefore, let’s say that your patient is suffering from a sepsis or septicaemia and that the patient went from having a pneumonia or perhaps even aspiration and there is so much damage that has taken place to the lung and alveoli, resulted in diffuse alveolar damage. We have acute respiratory distress syndrome. Now, this mostly does occur in adults, you can say that. And the only thing is that you need to keep in mind that could insults such as these also affect children? Sure it can. Toxic inhalation, drowning, all of this is then going to cause severe damage to the alveoli resulting in what? Diffuse alveolar damage. Welcome to acute respiratory distress syndrome which is then going to manifest as a pulmonary shunt. The clinical manifestations of diffuse alveolar damage can be seen in systemic or non-pulmonary. So, from this, let’s take a look at other important causes. Sepsis is probably the most common cause of acute respiratory distress syndrome. At some point, we will then transition into a more specific neonatal respiratory distress syndrome in which the most common cause there, well, we will walk through, but one of it, of course, being premie, meaning to say premature baby. 02:29 Next, pancreatitis, trauma and burns. Anyone of those actually could result in a condition called third spacing as well. For example, pancreatitis and burns are big ones. How many compartments do you have in your total body water? Two major compartments - ICF and ECF. 02:49 The fluid should be remaining in one of those two compartments. What if you pathologically then introduce a third compartment? Really? You can do that? Yeah, you can. If your patient is suffering from pain. Where? Oh, here doc. In my stomach. Anywhere else? Yeah, it actually hurts in my back too. Hmm, well high in your differential and then you find your lipase to be elevated, you have pancreatitis. And pancreatitis causes what? Well, at some point, you could then accumulate fluid in third compartment that has been introduced pathologically and your patient will have hypotension. In addition with pancreatitis, what are you looking for? Oh, lipase. What are some of those other important exocrine enzymes of the pancreas? They include your trypsin, chymotrypsin, elastase, lipase, amylase. All of those are what? Exocrine pancreatic enzymes. Having fun yet? All these enzymes might do what? Uh-oh, they might enter the blood stream, might go up into lungs and then may bring about damage. Welcome to ARDS. Fascinating. 03:55 Trauma, burns, all of these could result in acute respiratory distress syndrome. So, severe pneumonia we talked about, may be inhalation of toxic and such, but understand, the most common is the fact that you’ll go into sepsis. Idiopathic known as Haman-Rich syndrome, if you must memorise. 04:14 Acute respiratory distress syndrome results in hypoxic respiratory failure. There is going to be a significant V/Q mismatch. What does that mean? Well, I began by saying that there is going to be a pulmonary shunt, no doubt. What does that actually mean to you, clinically? Meaning to say that your patient is receiving oxygen, but you do not find significant improvement of this hypoxemia. Fascinating. Why? Because the alveoli is gone, it ain’t there, it’s collapsed. That's the significance, clinically, of your pulmonary shunt, but you knew that already and is it possible that you might be introducing pathologic areas of dead space units? Yes you may, yes you may. But the main thing here is pulmonary shunt. In addition, well now that you have damage taken place to the lungs, you tell me, what does it say? Cardiac type of damage or cardiogenic type of damage to your lung or was it a noncardiogenic type of damage to your lung? Obviously, a noncardiogenic. What does that mean? I had damage. What is the most common cause? Well, maybe sepsis, maybe aspiration, what have you. And if there is damage taking place in acute nature to the lung, understand that now, I am going to have an acute inflammatory response. Okay. That acute inflammatory response tumor, calor, rubor, swelling. So, therefore, I have increased capillary permeability;Tumor - swelling. Rubor – redness, calor - heat dissemination. Obviously, you are not going to feel the heat, but inflammation is taking place and endothelial cells are then going to then space out and then you have increased capillary permeability. So therefore you tell me, what kind of fluid? Protein rich or protein poor? Good. Protein rich. Welcome to exudate. This in turn leads to stiffening of the lung and decreased compliance and the more that you have leakage of fluid and its exudate in the interstitium, you can only imagine that the lung has now lost the ability to do what? Distend. Welcome to non-compliance. 06:18 What are we looking at here in the chest X ray? You will notice especially on the right side of the chest, that you find quite a bit of opacity there. That is because of the alveoli, in fact, is dead but, I would have to tell you this. As a medical student perhaps or if there is lack of exposure to chest X-rays, looking at this, well, all you know is that there is increased opacity, you definitely do not find calcifications here and the fact that you find the issue taking place at interstitium, hmm, tells you that is interstitial lung disease. 06:50 I mean to say that it seems like it is interstitium. The alveoli, if they are dying, they are going to appear getting a little bit more opaque. And so therefore, you might get a chest X-ray in which it is going to focus on the fact that the alveoli is then being collapsed. 07:05 But, always go back to make sure that your history coordinates with the findings of your image. Remember, these things you just use to complement your diagnosis. 07:16 Let’s take a look at important differential diagnosis for you in ARDS. Pulmonary edema.
About the Lecture
The lecture Acute Respiratory Distress Syndrome (ARDS): Pathogenesis by Carlo Raj, MD is from the course Disorders of the Pulmonary Circulation and the Respiratory Regulation.
Included Quiz Questions
Which of the following is correct about acute respiratory distress syndrome?
- Diffuse alveolar damage
- Diffuse bronchiolar damage
- Diffuse capillary damage
- Diffuse interstitial damage
- Diffuse connective tissue damage
What is idiopathic acute respiratory distress syndrome called?
- Hamman-Rich syndrome
- Hallermann-Streiff syndrome
- Reye’s syndrome
- Meigs syndrome
- Horner syndrome
What is the most common cause of acute respiratory distress syndrome in adults?
- Sepsis
- Pneumonia
- Trauma
- Toxins
- Drowning
Which of the following is not true regarding the association of acute pancreatitis and acute respiratory distress syndrome?
- Release of endocrine pancreatic enzymes
- Release of exocrine pancreatic enzymes
- Third-spacing of fluids
- ARDS becomes the final common pathway.
- Exudate
Which of the following is not seen in acute respiratory distress syndrome?
- Transudate
- Increased dead space
- Exudate
- Decreased compliance
- Shunting
Author of lecture Acute Respiratory Distress Syndrome (ARDS): Pathogenesis

Carlo Raj, MD
Customer reviews
2,1 of 5 stars
| 5 Stars |
|
4 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
1 |
| 1 Star |
|
10 |
Dr. Carlo Raj, i like a lot the way you expose the lectures. You explain everything in very understandable way
Thank u so much Dr Raj. It was a very good lecture.
13 customer reviews without text
13 user review without text
