Playlist
Show Playlist
Hide Playlist
Pediatric Diarrhea

-
Slides GD Pediatric GI.pdf
-
Download Lecture Overview
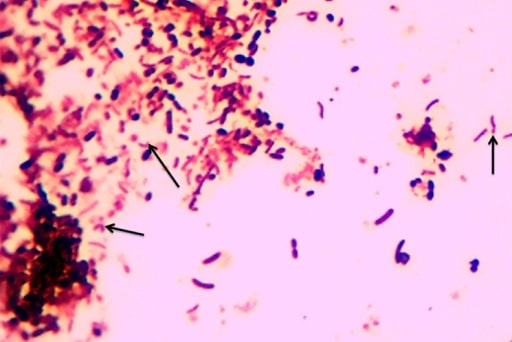
00:00 Our topic now, we'll move to pediatric diarrhea. 00:06 Obviously the definition will be increased stool output, and you're definitely worried about in a child of losing electrolytes. 00:16 Maybe acute or chronic. 00:17 Etiology maybe infection or perhaps malabsorption. 00:20 We'll talk about differentials in a little bit. 00:23 Mechanism may be osmotic. 00:26 Stool volume depends on the diet and decreases with fasting. 00:30 By osmotic, we mean that there is not enough absorption, therefore, creating an osmotic environment in the intestine, therefore, pulling in water resulting in diarrhea. 00:42 Or perhaps it might the secretory type. 00:44 So two different types of diarrhea that may be seen in the pediatric population. 00:50 In secretory, the stool volume is increased and does not vary with diet. 00:55 That, you want to pay attention to. 00:57 In osmotic, the less that the child eats, there's less of a chance of stool output being increased. 01:04 If it's secretory, then there is increased – let's say, it's something like a Vibrio cholera infection, a secretory type of diarrhea, regardless as to how much consumption by the child of food, it's not going to change the amount of stool volume. 01:21 That will continue to be persistent. 01:23 You pay attention to that, please. 01:28 Let us now go into differentials and etiologies. 01:31 Viral, extremely common. 01:33 Of all the viral, rotavirus is the most common if you remember from microbiology, especially during winter months up in the north. 01:42 This is when the children are playing and they really don’t play outside too much and maybe perhaps the parents are dropping their children off in day care centers, and because of lack of exposure to the outside world, they're kind of closed in these closed environments. 01:58 It's easy, really easy for infections to be taking place over and over and over again. 02:04 You'll see this during the winter months quite a bit. 02:08 Also, take a child onto a cruise in general, meaning to say, Norwalk virus and I've kind of made light of this earlier, and I talked to you about going on a Norwegian cruise line. 02:21 And the reason I say that is because Norwalk viruses are viruses that are found on cruise ships. 02:31 And you can have a child or an adult who consumes from the buffet that has now been infected by the virus called Norwalk. 02:40 The most common viral cause of gastroenteritis is Rota. 02:45 Cruise ships, Norwalk. 02:48 Bacterial causes of pediatric diarrhea. 02:51 And I'll walk you through this in greater detail coming up In which I will show you signs and symptoms. 02:56 E. coli, quite common, especially pathogenic. 03:00 Salmonella, look for a child having pets, and by pets, maybe perhaps even reptiles. 03:06 Shigella. Campylobacter, extremely common. 03:09 Yersinia. 03:10 Yersinia will be interesting to you. 03:13 And for that -- And the reason I say that is because It shares -- the infection shares similarities with certain systemic pathologies such as inflammatory bowel disease or perhaps even, what do we call – What we call pseudoappendicitis and Clostridium. 03:31 Parasitic. 03:32 Entamoeba histolytica, giardia. 03:34 If you take the child, maybe perhaps, he's accompanying you on a hiking trip And during that hike, there's every possibility that there might be consumption of water. 03:44 that has been contaminated by giardia and cryptosporidium. 03:49 Remember that cryptosporidium is usually a parasite that is going to affect a patient whose immune system is not fully developed. 03:59 Remember in HIV patients, the most common cause of diarrhea, is Cryptosporidium parvum. 04:05 This is not a child with HIV, that is not what I'm saying. 04:08 This is a child whose immune status is not fully mature yet. 04:12 Therefore, maybe susceptible to cryptosporidium type of infections. 04:18 Pediatric diarrhea, important gastroenteritis differentials. 04:24 Pediatric diarrhea, important gastroenteritis differentials. 04:28 The rotavirus, watery diarrhea for 7-10 days, approximate week. 04:33 Also, in addition to diarrhea, it may also present with vomiting and because this is a virus, it's supportive therapy. 04:41 And by supportive therapy, it would mean that you have to make sure that the child-- First and foremost, if there's diarrhea and there's vomiting in a child, my goodness, you want to make sure that the hydration status of your child is properly taken care of. 04:56 E. coli. 04:58 Here, we have enteropathogenic E. coli. 05:00 Nurseries and daycares. 05:01 Once again, think of winter months in which the children are playing close together, And so therefore may then spread infections. 05:09 Salmonella. 05:10 Egg, poultry, milk, reptiles, pets. 05:15 Salmonella, quite common. 05:18 Shigella. 05:20 Contaminated food and look for the child who actually maybe experiencing seizures. 05:26 S – Shigella. 05:27 S- Seizures. 05:29 Specific pathological clinical manifestations of some of your infections. 05:36 Continuing. 05:37 Campylobacter, extremely common Contaminated food, extremely common. 05:41 Campylobacter jejuni. 05:43 Yersinia I explained earlier that what you're paying attention to would be how it behaves like systemic pathologies such as, be careful not to confuse it with inflammatory bowel disease or pseudo-appendicitis. 05:59 And by that, we mean that there might right lower quadrant pain, kind of like appendicitis. 06:04 Yersinia, also transmitted by pets, contaminated food, and associated with arthritis and rash, look for extra-intestinal manifestations with Yersinia big time. 06:17 Clostridium, what happens here? Usually significant. 06:21 Maybe perhaps prior antibiotic use. 06:25 Clostridium. 06:26 Staph aureus, extremely quick. 06:28 twelve hours after ingestion of let's say those food items that may then contain egg products such as mayo, all right? So for example, potato salad and such. 06:41 Diagnosis. 06:43 You're going to recover the organism in the stool and enzyme immunoassays. 06:48 Pretty straight forward. 06:48 Examine the stool when there's pediatric diarrhea. 06:53 Supportive therapy, only for viral. Only for viral. 06:56 Remember, there are no viral antibiotics. 07:00 No such thing. 07:01 And because of all of the vomiting and loss of fluid, you're worried about the hydration status. 07:08 For salmonella, antibiotics are indicated only for ages less than 12 months. 07:14 If the patient is in a toxic state, if there is disseminated disease, or they are immunocompromised There is also important to note, that for salmonella typhi Trimethoprim/sulfamethoxazole actually prolongs to the carriage state. 07:27 For shigella, Azithromycin is the prefered agient, if the antibiotics sensitivity is not known. 07:32 This is due to hyresistance patterns. 07:34 For Campylobacter, antibiotics are reserved for severe disease or patients that are immunocompromised. 07:40 The remmended agient is erythormycin. 07:44 Yersinia. 07:44 Less than 3 months once again, antibiotics So you're worried about children and you want to bolster their immune system. 07:51 Also with Yersinia, worried about septicemia. 07:55 Aminoglycosides or third generations cephalosphorins are a possibilities for Yersinia. 08:01 The difficile, oral metronidazole is your drug of choice. if you find your patient to be and at some point in time, if you find your patient to be resistant to metronidazole, you should be thinking about oral vanco. 08:14 Entamoeba, metronidazole. Giardia, metronidazole. 08:17 In general, if we think about parasites, you should be thinking about metronidazole.
About the Lecture
The lecture Pediatric Diarrhea by Carlo Raj, MD is from the course Pediatric GI Pathology.
Included Quiz Questions
Of the following choices, which viral cause of diarrhea is the MOST common in the pediatric age group?
- Rotavirus
- Clostridium
- Coronavirus
- E. coli
- Adenovirus
A 3-year-old boy goes to day care and develops diarrhea after eating fresh fruits and vegetables there. What is the mode of transmission of the infectious agents?
- Fecal-oral route
- Exposure to aerosols
- Exposure to new food diet
- Passing through saliva
What is a common risk factor for enteropathogenic E. coli?
- Day-care attendance
- Playing in freshwater streams
- Keeping reptiles as pets
- Consuming contaminated eggs
- Exposure to contaminated milk
Which of the following organisms has reptiles as a common risk factor for causing diarrhea?
- Salmonella
- Shigella
- Campylobacter jejuni
- Rotavirus
- Vibrio cholerae
A 10-year-old boy presents with abdominal pain and rash. He then develops joint pain and diarrhea over the next few days. The parents thought it was appendicitis and approached the doctor. However, the appendix was normal on ultrasound scan. Which of the following can treat the possible organism?
- Antibiotics
- Antivirals
- Antituberculous drugs
- Antifungals
- Antiparasitic drugs
Which of the following statements regarding pediatric diarrhea is FALSE?
- Secretory diarrhea is always infectious.
- In osmotic diarrhea, the stool volume increases by absorption of more water into the bowel.
- Osmotic diarrhea decreases when fasting is performed.
- In secretory diarrhea, the stool volume does not depend on the diet.
- In secretory diarrhea, the stool volume increases due to the production of mucus.
Which of the following is the drug of choice for the treatment of pseudomembranous colitis diarrhea in the pediatric population?
- Oral vancomycin
- IV vancomycin
- Co-trimoxazole
- Ampicillin
- Supportive therapy
A 10-year-old boy presents with chronic diarrhea. A colonoscopy shows multiple, golden-brown, membrane-like structures. The patient was given a complete course of metronidazole but did not respond to it. What is the next BEST step of management?
- Provide a complete course of vancomycin.
- Repeat the complete course of metronidazole.
- Give a short course of vancomycin.
- Give the alternate antibiotic of amoxicillin.
- The condition is self-limiting and does not require further treatment.
Author of lecture Pediatric Diarrhea

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
