Playlist
Show Playlist
Hide Playlist
Introduction & Hypothalamus – Adrenal Cortex


-
Slides AdrenalCortex EndocrinePathology.pdf
-
Download Lecture Overview
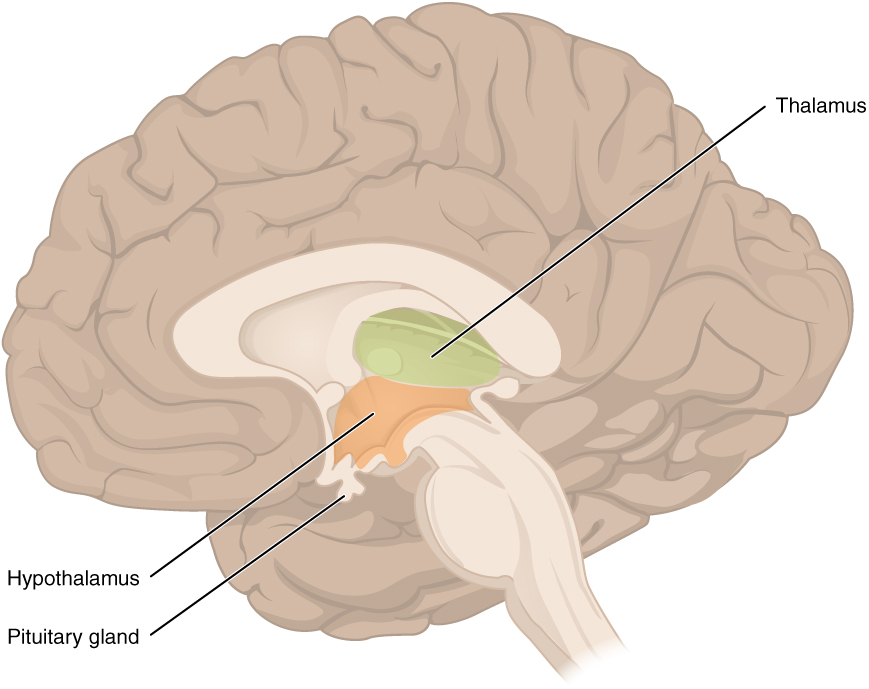
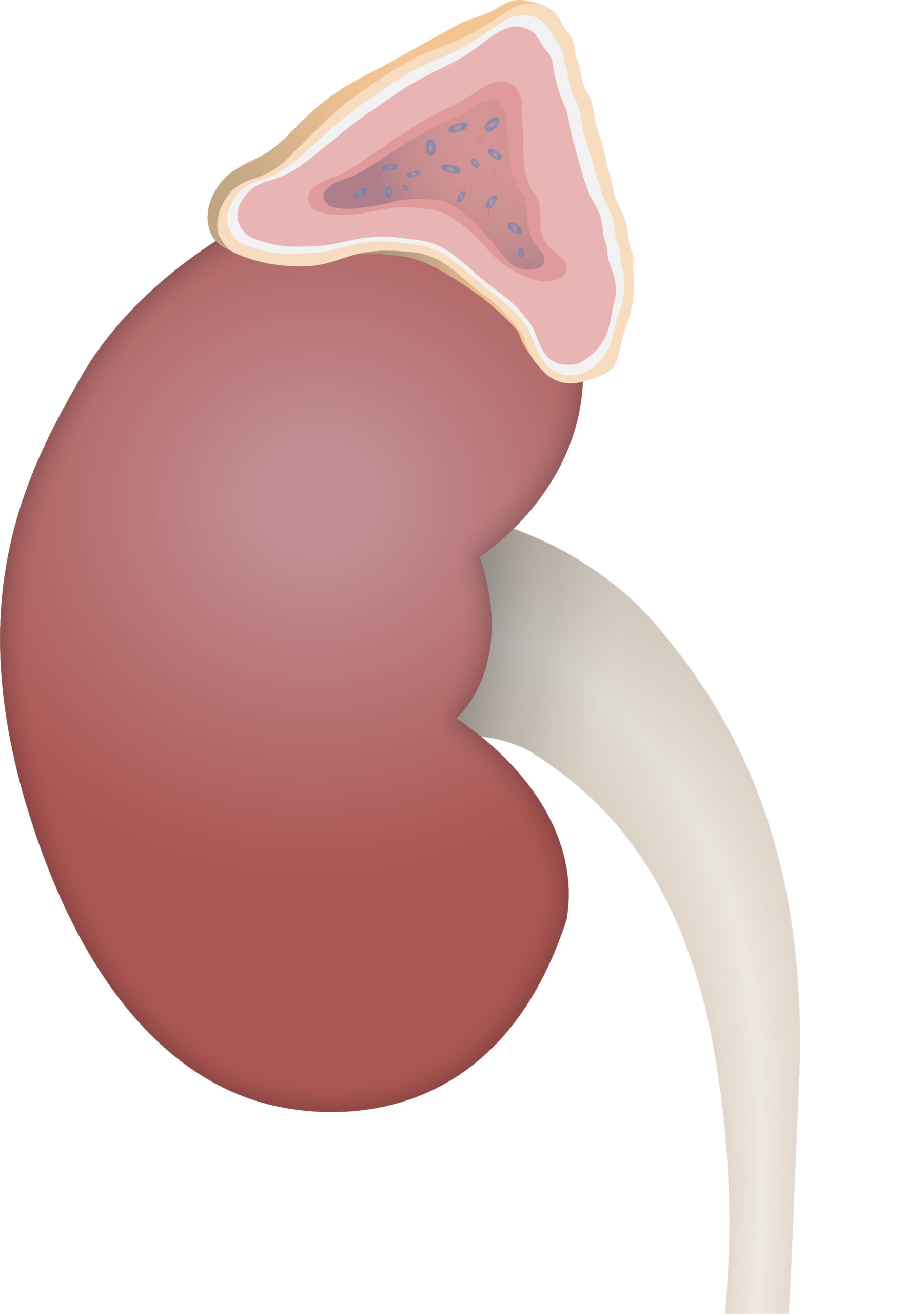
00:01 Welcome to our discussion of adrenal gland pathology. 00:04 Before we begin, we’ll take a look at the adrenal cortex and do a brief review. 00:10 Illustration here on your right, you divide your axis into two components like you would with many of the other axes. 00:21 For example, the hypothalamus and the pituitary play a role in many, many, many axes including that of your gonads, hypothalamus, pituitary, gonadal axis, we’ll talk about later, hypothalamus, pituitary type of thyroid axis that we have discussed. 00:40 Here, we have the hypothalamus, pituitary, adrenal axis. 00:47 From the hypothalamus, the pattern that we’ve established over and over again is that you release your releasing hormones. 00:54 This then triggers the pituitary to then release the appropriate hormone where, in this case, it will be ACTH and the target organ for ACTH would in fact be your adrenal cortex. 01:06 Let’s dive into this a little bit deeper. 01:12 From your hypothalamus, we have the corticotrophin releasing hormone which then acts upon your anterior pituitary here and when it does so, it triggers the breakdown of your pro-opio, the opioid will be beta endorphin, the melano would be the melanocyte stimulating hormone and the corticotroph would obviously be our ACTH, our primary focus of our entire discussion. 01:44 ACTH will then be released into circulation and then the receptor that you see down at the bottom would represent the receptor upon the adrenal cortex. 01:56 You are now down in your abdominal region. 01:59 In the box, what you are seeing here is the control of ACTH and when ACTH would play a role especially its responsibility would be cortisol release. 02:13 Sure, ACTH has a minor influence upon aldosterone synthesis and I say minor because for you to form a fully pledged or fully mature aldosterone, that’s a discussion that we’ll have in a little bit, but ACTH is definitely responsible for cortisol synthesis. 02:34 That cortisol is incredibly important during those times of stress… what kind of stress? Well, how about fasting when you are hungry, infection, and any time that you’re fasting, you know that you then have to follow your gluconeogenic pathway, so cortisol and glucagon will always have permissive action. 02:57 If at any point in time you’re missing cortisol, your patient now is at risk for death. 03:04 So, absolutely necessary for sustenance of life. 03:10 When is cortisol released? At the end of the day, when you feel tired is when your cortisol levels are the lowest. 03:18 Around midnight and thereafter when you’re sleeping at night is when your cortisol levels start rising. 03:26 Wake up in the morning, it is at its highest level; we call this number one, diurnal rhythm. 03:33 It’s imperative that you know the normal rhythm of your cortisol because you will be responsible for understanding how the dexamethasone suppression test actually functions. 03:46 You will be responsible for that, I’ll walk you through it. 03:51 It is a stress hormone and cortisol inhibition. 03:54 If you take a look at the picture on your left, you’ll notice that cortisol has inhibitory effect or feedback upon your hypothalamus and the anterior pituitary inhibiting the release of those respective hormones. 04:08 ACTH… do not forget will work through your GS-protein therefore, we have cyclic AMP as its signal transducer. 04:19 Here, the adrenal cortex down the abdomen… what I would like for you to do is establish a pattern of what this looks like anatomically granted these are biochemical pathways. 04:33 But, from left to right, you will be moving from superficial deep side, literally I need you to think of the adrenal gland and our focus only in this discussion will be with the cortex, right? Whereas the medulla will be responsible for epinephrine… that discussion to be had at a later time. 04:55 Now, with the cortex, you were moving from superficial to deep, I need you to move from the left… in the left column and at this point, all we’re doing is an overview. 05:08 We will get into greater detail where you will be able to see these specific substrates and enzymes, but I just want you to understand the pattern here. 05:18 We have the zona glomerulosa, we’ll then refer to what’s known as the zona fasciculata responsible for cortisol release and then finally reticularis which is that green box that you see way to the right and that is your reticularis. 05:34 That is the deepest structure of the adrenal cortex. 05:37 So, those are the three columns that we’ll be focusing upon, each one of those columns play pivotal role with synthesis of various adrenocortical hormones. 05:52 Adrenal cortex in the cell, where are we? Okay, now, the same pattern, but now we’re blowing it up. 05:57 First, you’ll notice ACTH binding to a receptor, we have GS-protein, cyclic AMP. 06:03 It’s important that you know the enzyme here, understand that cholesterol is brought into the adrenal cortex. 06:11 Cholesterol from biochemistry, carried by LDL and I will give you a little bit of an overview to show you the LDL receptors bringing in the cholesterol. 06:20 That is important for you to know because at any point in time, if LDL receptors aren’t working properly such as type II hyperlipidaemia, huh, you can’t even bring in cholesterol into your-into your organ. 06:31 Anyhow, cholesterol is the-is the omnipotent factor here that is responsible for synthesis of adrenocortical hormones. 06:41 So, begin there, please. 06:43 Next, the rate limiting enzyme that we’ll refer to here is called desmolase responsible for breaking down your cholesterol into pregnenolone. 06:52 Now, where are you in the adrenal cortex? This first column and all we’re doing is the first step here is the zona glomerulosa. 07:03 You tell me what is zona glomerulosa responsible for synthesizing? Good, aldosterone. 07:11 However, as I said, ACTH will kick-start the synthesis of aldosterone, but it will not complete the job, that’s important because you know that aldosterone and its major feedback is going to be with whom? You’ve heard of the acronym RAS, right? Renin… angiotensin… aah, aldosterone, so renin clinically will be the most important feedback for you with aldosterone. 07:39 Let’s move on. 07:41 We’ll then going to move from the glomerulosa into the fasciculata which is that blue box that you see there. 07:49 Here, there’s an enzyme that will take you from the glomerulosa to the fasciculata this is then noted and abbreviated as 17-alpha-hydroxylase. 07:59 So, 17-alpha-hydroxylase is an enzyme that allows you to go from your glomerulosa into the fasciculata… that must be understood. 08:11 At some point in time, obviously, we’ll start talking about pathologies in which you’re deficient or your patient is deficient of certain enzymes. 08:21 17-alpha-hydroxylase deficiency could be a possibility, but I’ll tell you which ones to focus upon first. 08:28 Something else that I want you to focus on now that we’re officially in our fasciculata, you have something called hydroxy… you see that? So, this is hydroxypregnenolone that becomes important for us and it’s 17… 17 hydroxypregnenolone. 08:43 That becomes important for us because of... just keep that in mind, they could ask you something about what you might find in the urine and I’ll give you a table in which you will… we’ll take a look at that further. 08:56 And then you go from your fasciculata down into the green box there, that would be the deepest of the layers and that would be your reticularis and that DHEA stands for dehydroepiandrosterone. 09:12 Your focus there would be the “A” because the reticularis is responsible for synthesizing androgen type of hormones. 09:20 Androgen, not estrogen, so any time that you would find, let’s say, excess activity of the reticularis, what’s your patient going to look like? If it’s a female, a young girl… masculinization, right? If it’s a male, well, he’s already a boy, but he might then have or experience precocious puberty. 09:45 Let’s move on. 09:46 We’re going to add bit by bit by bit so that you remain focused and organized with what is happening. 09:53 Our next enzyme here, I’ll tell you exactly what to take a look at here would be where we left off in the glomerulosa, identify that first and that would be your leftmost column. 10:04 We already discussed desmolase and pregnenolone and in the previous discussion, we went from pregnenolone into the fasciculate. 10:13 What’s the name of that enzyme called? 17-alpha-hydroxylase, that’s what that bar stands for, that bar that you see there is an enzyme. 10:23 But, what if you want to go through each of the columns? What if you want to go from… please identify pregnenolone. 10:30 Next, I want you to then identify your progesterone. 10:35 How did you convert your pregnenolone to progesterone? Very important that you know this enzyme, it’s called 3-beta hydroxysteroid dehydrogenase. 10:43 It’s abbreviated here as being 3-beta, at least be able to identify 3-beta. 10:48 3-beta hydroxysteroid dehydrogenase, where is this enzyme located? You see that bar horizontally, it is in the superficial most layer, the glomerulosa. 10:59 It is also in the fasciculate, it is also in the reticularis. 11:04 Hence, you see the bar going all the way through the cortex. 11:08 What does that help you do? It helps you go through each layer, meaning to say you’ll go within the glomerulosa, you convert your pregnenolone into progesterone. 11:18 Next, I want you to go into the blue box, that’s your fasciculata. 11:23 We were at hydroxypregnenolone, identify that with the help of the enzyme 3-beta hydroxysteroid dehydrogenase, you convert it into 17-hydroxyprogesterone and then finally reticularis. 11:35 I told you to focus upon the letter “A” because that then to you means an androgen, the androgen here would be androstenedione. 11:45 Our next enzyme that we’ll take a look at and ultimately the most important enzyme of all the enzymes so far, we’ll look at two… 17-alpha, 3-beta. 11:57 However, the most important enzyme and the reason I say that is because there’s a pathology that you know of known as congenital adrenal hyperplasia… congenital adrenal hyperplasia. 12:07 Who’s your patient? Congenital, child, so in utero, the child, the foetus never developed the enzyme. 12:18 There are three enzymes that might be deficient. 12:23 Of all the enzymes… actually, four to be technical, but at least know the most important one of all the enzymes that could be deficient in the adrenal cortex it is this one, this one, this one. 12:34 Which one is it am I referring to? 21-beta hydroxylase here abbreviated as 21-beta. 12:39 What does it do? Take a look. 12:43 That 21-beta hydroxylase... first and foremost, where do you see the bar? The bar is horizontal only located in the glomerulosa, only located in fasciculata, obviously not located in reticularis, so you don’t need it there. 12:58 Hence, the bar stops there. 13:00 What does it do? Ah, now, this is where it becomes important and really interesting because I’m going to add in your clinical application. 13:06 I’m going to show your patient or you’re going to imagine your patient here. 13:09 So, you take the… I want you to go with the glomerulosa, we’re at the progesterone. 13:16 From your progesterone, what does this enzyme help you convert to? 21-beta hydroxylase permitted you do convert into your DUC, D-U-C that stands for 11 deoxycorticosterone or 11-DUC… that you have to... you have to commit to memory. 13:35 It has a weak… physiologically, it has a weak mineralocorticoid activity… weak mineralocorticoid, physiologically. 13:44 Pathologically, completely different picture. 13:48 What does mineralocorticoid activity mean to you? It means reabsorbing sodium and water. 13:57 The operative element, the sodium. 14:00 You tell me if you’re reabsorbing, retaining more sodium, what does it affect? Blood pressure? Sure, and blood pressure meaning what? Systolic, diastolic, right? Blood pressure will be elevated when you’re retaining more sodium. 14:16 Let’s talk about this patient and our focus... and your focus should be on 21-beta hydroxylase. 14:22 Keep in mind that they could technically give you other enzyme deficiencies, but let me show you if you’re deficient 21-beta hydroxylase identify please, are you producing DUC? No, if you’re not producing any DUC, you sure as heck are not producing any aldosterone. 14:44 If you have no mineralocorticoid, what’s your blood pressure in your child? Decreased. 14:49 Okay, we’ll talk more about this later step by step by step so that you have a firm understanding of these enzymes and how they operate. 14:58 There’s another enzyme here. 15:00 We are now moving on to the blue bar which is 11-beta hydroxylase. 15:07 What does it do? Notice here, please, now at this point, we can move a little bit faster, I believe that you’ve established the pattern quite well. 15:14 So, in the glomerulosa, which is the first column on your left, which is responsible for all aldosterone synthesis, you’ll notice that this bar representing the enzyme is only in the glomerulosa and it’s only in the fasciculata. 15:28 Once again, why do you require it in the reticularis? You already have your androgen, so let it go, hmm? Next, where do we leave off in the glomerulosa? We formed our DUC, deoxycorticosterone. 15:41 Please be very careful because you will get answer choices in biochemistry in which your deoxycorticosterone might look like your deoxycortisol. 15:49 You see that in the blue box they look alike and you’re tired maybe perhaps when you’re taking the exam very easy that your eyes can get confused between those two. 15:59 Do not ever do that. 16:00 So, we’ll take our DUC and with the help of the enzyme 11-beta hydroxylase, we’ll then form our corticosterone and that corticosterone with the help of… here’s an enzyme called aldosterone synthase. 16:14 Aldosterone synthase, hmm, what’s responsible for stimulating aldosterone synthase? Well, if you know it’s aldosterone, what is its major feedback mechanism? Renin-angiotensin. 16:28 What kind of angiotensin? Angiotensin 2 stimulates aldosterone synthase so that you form your aldosterone… welcome to RAS. 16:38 We’ve completed our discussion of the glomerulosa, let’s move over into the blue box which is the fasciculata. 16:44 You’ll notice here that your deoxycortisol is being converted into cortisol and there’s a little stanza there that says that cortisol, remember, these are all adrenocortical hormones, these are all lipid soluble that will pass through the membrane and where is the receptor for your adrenocortical hormones located? Nucleus or cytoplasm? Good, cytoplasm. 17:07 And that’s what that paragraph says there. 17:10 In the meantime, take a look at the reticularis. 17:12 What are you producing? What kind of hormones? General theme… androgen, androgen, androgen. 17:19 This is an overview of your adrenal cortex and its major enzymes, your focus should be on 21-beta hydroxylase and I gave you one little clue here about your patient where, if your patient is deficient of the enzyme 21-beta, you are not producing any mineralocorticoid, your patient’s blood pressure is decreased. 17:35 I will tell you later as to why your patient will be… if-if-if your patient’s a female, the young girl will be virilised; where if it’s a male, then your child, the boy, will be experiencing precocious puberty. 17:51 I’ll tell you why. 17:52 For those of you who are ahead of me, you already understand this.
About the Lecture
The lecture Introduction & Hypothalamus – Adrenal Cortex by Carlo Raj, MD is from the course Adrenal Gland Disorders.
Included Quiz Questions
What is the CORRECT mechanism of ACTH secretion?
- CRH released from the hypothalamus acts on POMC in the anterior pituitary, which releases ACTH
- CRH released from the hypothalamus acts on the anterior pituitary to release POMC, which stimulates ACTH release from the adrenal glands
- POMC released from the hypothalamus acts on CRH in the anterior pituitary, which releases ACTH
- CRH released from the hypothalamus acts on the liver, which stimulates the breakdown of POMC, releasing ACTH
- CRH released from the hypothalamus acts on the anterior pituitary to release ACTH, which stimulates the production of POMC
What is required for the synthesis of adrenal hormones?
- Cholesterol
- POMC
- DHEA
- Epinephrine
- ACh
Where is aldosterone synthesized?
- Zona glomerulosa
- Zona fasciculata
- Zona reticularis
- Adrenal medulla
- Hypothalamus
Which enzyme is responsible for converting pregnenolone to progesterone?
- 3β-hydroxysteroid dehydrogenase
- Desmolase
- 17α-hydroxyprogesterone
- DHEA
- 17α-hydroxypregnenolone
Which enzyme will most likely be deficient in a child with congenital adrenal hyperplasia?
- 21β-hydroxylase
- 3β-hydroxysteroid dehydrogenase
- 17α-hydroxypregnenolone
- Desmolase
- DOC
What are the precursors of 11 deoxycortisol and corticosterone, respectively?
- 17-hydroxyprogesterone; 11-deoxycorticosterone
- Aldosterone; cortisol
- Cortisol; testosterone
- Testosterone; cortisol
- Aldosterone; testosterone
Author of lecture Introduction & Hypothalamus – Adrenal Cortex

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
this lecture covers almost everything I need to know to learn about th adrenal before stepping into its pathology
