Playlist
Show Playlist
Hide Playlist
Overview of Sedative and Hypnotic Drugs – Sedative Hypnotics

-
Slides Sedative and Hypnotic Drugs CNS Pharmacology.pdf
-
Download Lecture Overview
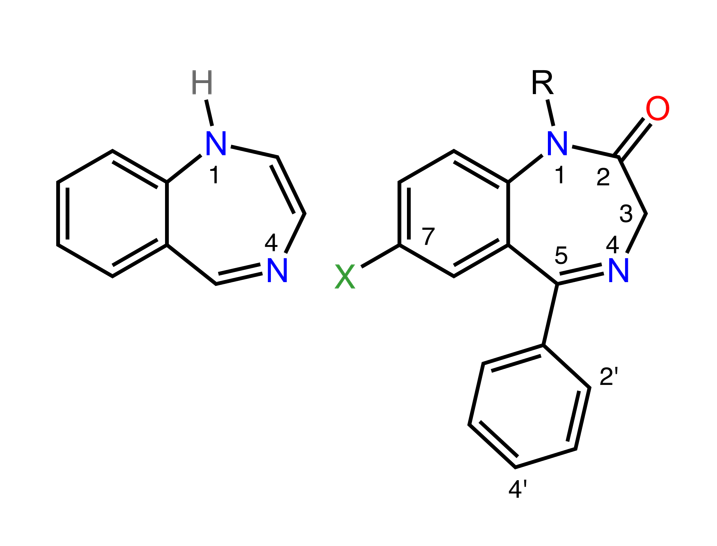
00:01 Hi, welcome to the pharmacology lectures by Lecturio. My name is Dr. PJ Shukle and today's lecture is going to be about the sedative and hypnotic drugs that we use in everyday clinical practice. Here is an overview of the medications that we are going to be covering in this section of the lectures. We have benzodiazepines which are probably the most commonly used of the sedative drugs out there. We also have barbiturates which are commonly more used in anaesthesia. 00:34 And we have atypical drugs that can be used in various forms and in various clinical scenarios. Benzodiazepines are often converted to active metabolites in the liver. Examples include diazepam and flurazepam. The important medications that you should know is really diazepam for your medication, but flurazepam is used a lot in clinical practice. One of the problems of these medications is that they can actually accumulate over several days. So one has to be very careful with these medications in using them on a day to day basis. Some of these benzodiazepines are conjugated outside the liver. 01:15 An example is lorazepam or oxazepam. Once again lorazepam is something that you should know for your exams. Oxazepam is something that we see more clinically. Now these particular drugs do not form active metabolites. Barbiturates are extensively metabolized in the liver. An example or a prototypical drug is the short acting secobarbital. Phenobarbital can be excreted in the urine unchanged. Phenobarbital is a longer acting version and it's often used in patients who have epilepsy. The unclassified drugs have rapid metabolism by liver enzymes and they have a shorter duration of action. 02:01 Most of the times we are using these drugs as sleep aids because they wear off by the morning. Here is a dose response curve for all of the medications in one graph. When you look at this graph you can see that at low dose, we just talked about sedation, disinhibition and anxiolysis which is the removal of the feeling of anxiety. At higher doses, we start to see hypnosis where we see loss of consciousness and reduction of awareness. Once we get into the anaesthesia range the benzodiazepines are used less and less. You can see that they sort of peak out at the anesthesia, hypnosis range. 02:41 Barbiturates however are fairly toxic. So they keep going up in the toxicity spectrum. So you can actually get medullary depression and coma. And many times we will use barbiturates to induce a coma in certain situations. Let's start off with sedation, disinhibition and anxiolysis. So obviously at this lower dose of the spectrum, anxiolysis and sedation is going to be mostly with the benzodiazepines. These are at low doses of both sets of drugs. Benzodiazepines are used far more frequently for anxiolysis than any other category. And the newer unclassified drugs are starting to come into play with this particular type of therapy. And you are starting to notice that the newer drugs, and the more new the flatter the curve, have a flatter curve which means that they peak out in the anxiolysis spectrum. Going back to our curve, let's talk a little bit more about antiseizure activity. Now antiseizure activity is present with both your benzodiazepines and your barbiturates. It's present at very low levels of barbiturates like phenobarbital as I mentioned before. 03:57 And it's present at higher doses of the benzodiazepines like lorazepam and midazolam. When we move into the hypnosis part of the spectrum, we start to see the benzodiazepines tailing off. Benzodiazepines can induce sleep. And rapid eye movement is often reduced, so people will get fewer dreams when they are on benzodiazepines. Now when you stop taking benzodiazepines there is a rebound effect with respect to your REM sleep, rapid eye movement sleep, and people will become hyper-REM, they will have more REM sleep. And they will have very vivid dreams and sometimes they will actually have nightmares. 04:40 As you get into the newer agents, we are starting to see fewer and fewer side effects. So a good example of that kind of a drug is zopiclone. We use it for insomnia, it has a very rapid onset of action and it has minimal daytime cognitive impairment. 04:58 This is a very good drug for use in insomnia and it's essentially replacing the older Ativan, which is lorazepam or Versed. It's replacing all of those old medications with these new medications because of their efficacy and lack of symptoms. Let's move on to the anaesthesia spectrum of our sedative hypnotic drug. You can see that the curve is flattening out with the benzodiazepines. Those benzodiazepines are great for certain types of anesthesia induction but for long term anaesthesia induction, we're using more barbiturates as time goes on. Anesthesia refers to a complete loss of cortical function. 05:39 You have amnesia, you have suppressed reflexes, you can have anterograde amnesia and you can actually have it with some of the benzodiazepines. Now we are going to talk about something called date rape or rape drug under toxicology, so keep that in mind with the benzodiazepines. Now, in the operating room we are using a lot of barbiturates. In the intensive care unit we use a lot of benzodiazepines. In the operating room, one of the most common barbiturates used is thiopental. Now short term sedation with benzodiazepines is excellant. So when I was working in the intensive care unit, I would often use IV Ativan or IV Lorazepam to sedate my patients for rapid sequence induction and intubation. Many other anaesthetist seem to prefer intraveneous diazepam, I preferred lorazepam. Whatever you choose, it doesn't really matter. Just recognise that these are the two main agents that we use intraveneously for short term sedation. Let's move on to the top of the spectrum. 06:48 We are now talking about medullary depression and coma. And you can see that this is starting to become the sole province of the barbiturate class of medications. So medullary suppression and coma means that these patients often will have a respiratory arrest. 07:04 They will develop low blood pressure because they have lost a lot of that sympathetic tone. There can be cardiovascular collapse if you are not administering the medications properly and it can also result in death.
About the Lecture
The lecture Overview of Sedative and Hypnotic Drugs – Sedative Hypnotics by Pravin Shukle, MD is from the course CNS - Pharmacology. It contains the following chapters:
- Overview of Sedative Hypnotics
- Metabolism
- Dose-response Curve for Medication
Included Quiz Questions
Which of the following statements best describes the role of benzodiazepines in clinical practice?
- Benzodiazepines are commonly used for anxiolysis and tend to decrease REM sleep, leading to fewer dreams.
- Benzodiazepines are primarily used for inducing coma in intensive care settings.
- Benzodiazepines are used mostly for rapid sequence induction and intubation.
- Benzodiazepines are not used for sedation due to their high toxicity profile.
- Benzodiazepines are mostly used in replacing older barbiturates for long-term anesthesia induction.
Which medication is appropriate for insomnia with minimal risk of daytime cognitive impairment?
- Zopiclone
- Lorazepam
- Diazepam
- Phenobarbital
- Flurazepam
Author of lecture Overview of Sedative and Hypnotic Drugs – Sedative Hypnotics

Pravin Shukle, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I chose this coz am able to memorise. Facts about the sedatives and hypnotics
