Playlist
Show Playlist
Hide Playlist
Acute Respiratory Distress Syndrome (ARDS): Signs, Symptoms, Definition, Treatment

-
Slides ARDS RespiratoryPathology.pdf
-
Download Lecture Overview
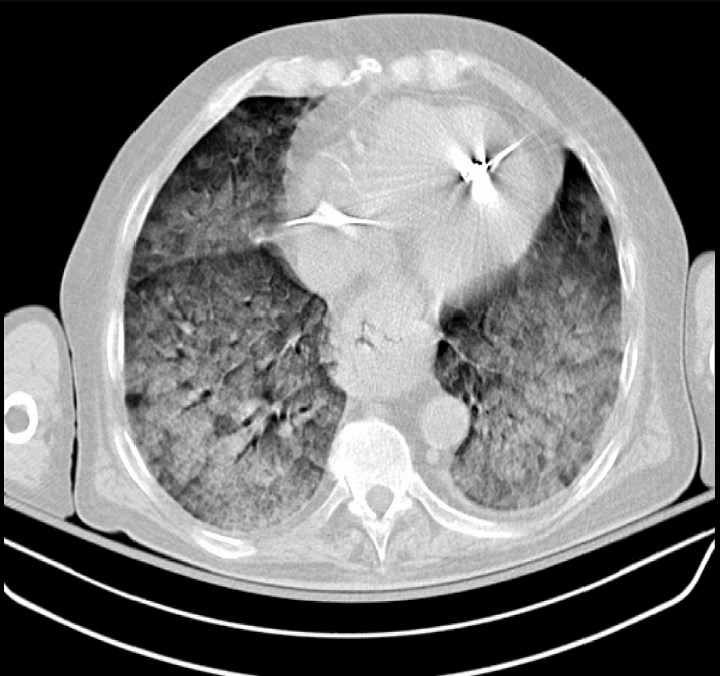
00:00 Let’s move on. Signs and symptoms of ARDS. Pretty straight forward now. So, once we have got through acute type of respiratory distress syndrome, we talked about sepsis being a very common cause, could be aspiration, toxic inhalation, pneumonia, and so forth. We talked about neonatal respiratory distress syndrome. We talked about tachypnea and we talked about surfactant deficiency. Most patients present similarly and present with tachypnea, hypoxia, tachy. Early, 12 to 24 hours. 00:35 Next, well if there is a severe V/Q mismatch, then you can expect, take a look and focus upon a widened A-aO2 gradient. As a rule of thumb, say that you are about to take your exam and you feel stressed. This is what you want to take in mind. A-aO2 gradient normal, if you have a pathology, outside of lung. A-aO2 gradient widened, when you have a pathology, inside the lung. For example, is this in the lung? Oh, absolutely. What about the chest X-ray? I will show you that. Diffuse alveolar infiltrate. It may, to a layman, it may, perhaps to a novice, be confused with interstitial lung disease. So, you need to close your eyes and think about what an alveolar looks like and if that is to be collapsed, then that’s what’s going to be found on chest X-ray. What about ABG? Marked hypoxemia. 01:33 Here, pay attention. From the very beginning, I have been saying that that this is a pulmonary shunt. Shunt, why it that important? Clinically, you give oxygen, but the patient does'nt find to be, or does'nt find significant improvement because of the shunt. But, you still have to give oxygen. Is that clear? Next, mechanical ventilation indicated decrease in pulmonary compliance. So, mechanical ventilation indicates that the pulmonary compliance has gotten so, so low and the lung is so very stiff that the only method by which this patient can now breathe is through mechanical ventilation. 02:09 Next, what about the pulmonary arterial catheterisation? Pay attention. Where is my damage? To lung. 02:18 Is this cardiogenic or noncardiogenic damage to the lung? Noncardiogenic. So, tell me about your left ventricular pressure. Normal. Understood? If you did a pulmonary capillary wedge pressure, do you want the differential that I showed you? Go back and take a look. The differentials of ARDS and I gave you pulmonary edema and I gave you the one with sepsis, in ARDS. Right? And during that time, in ARDS, you would also find your pulmonary capillary wedge pressure to be normal. Be careful, clinically, these things become very important for us. 02:55 Acute onset. Diffuse bilateral infiltrate. Your FiO2, well, it depends. Here, on a ratio less than 300. Definitely, your aO2 is going to be severely compromised. When your ratio is decreased, the numerator is decreased. Origin of edema, not fully explained by heart failure or volume overload With ARDS, you have to be able to manage your patient properly, no joke, ICU. You always try to get to correcting the underlying cause. May be it is sepsis, maybe it is aspiration, things we have talked about. Always look for mechanical ventilation, if the compliance is so low that the patient is not able to breathe. Remember, this was a big deal in neonatal respiratory distress syndrome where maybe you were thinking about giving CPAP, continued positive airway pressure or PEEP, positive end expiratory pressure. PEEP is used on the ventilator to splint open the alveoli, help oxygenate, low tidal volume ventilation, to minimize the ventilator trauma and conservative fluid management.
About the Lecture
The lecture Acute Respiratory Distress Syndrome (ARDS): Signs, Symptoms, Definition, Treatment by Carlo Raj, MD is from the course Disorders of the Pulmonary Circulation and the Respiratory Regulation.
Included Quiz Questions
Which of the following supports the diagnosis of acute respiratory distress syndrome?
- Increased A-a O2 gradient
- Increased left ventricular pressure
- Lobar consolidation on chest X-ray
- PaO2/Fi02 ratio > 300
- Indolent onset
Which of the following is involved in the pathophysiology of acute respiratory distress syndrome?
- Surfactant dysfunction
- Hypoventilation
- Cardiogenic pulmonary edema
- Decreased pulmonary arterial pressure
- Increased lung compliance
Author of lecture Acute Respiratory Distress Syndrome (ARDS): Signs, Symptoms, Definition, Treatment

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
He explains it well without any stress just like a pro
