Playlist
Show Playlist
Hide Playlist
Aortic Stenosis: Pathogenesis

-
Slides ValvularHeart DiseaseAorticStenosis CardiovascularPathology.pdf
-
Download Lecture Overview
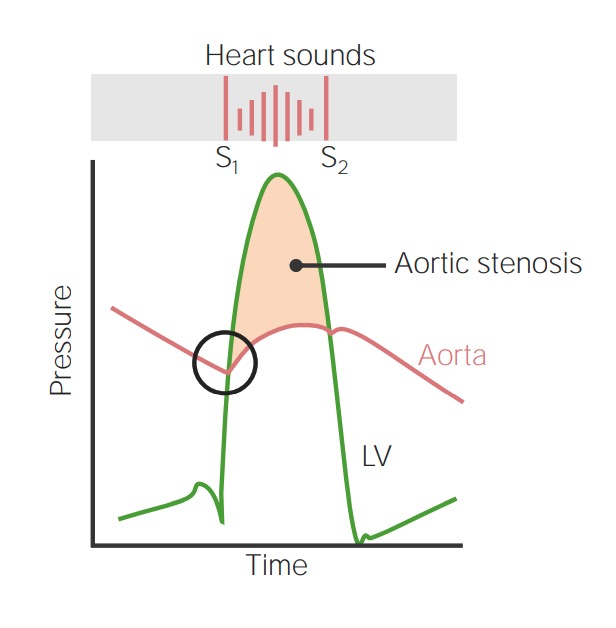
00:02 Begin with aortic stenosis. So this referred to a few times. How is the patient feeling? Walking through the door and your patient tells you, well I gave you that patient earlier. It was 32 years of age with aortic stenosis. How is it possible that 32 year old is having aortic stenosis? How is that possible that the aortic valve has already undergone so much damage that is now accumulating dystrophic calcification? In basic pathology, we talked about the differences between dystrophic calcification and metastatic calcification. You have done that plenty of times. What is the difference? Dystrophic calcification would be damaged, D; dystrophic D, damaged tissue occurs first. Where is the damaged tissue here? The aortic valve. So you have normal amounts of calcium that deposits on damaged tissue resulting in, well what kind of characteristic would calcium then give that tissue when it starts accumulating? Rigid, hard. So now we have an aortic valve, which is hardened due to dystrophic calcification, but still doesn't answer the question why a 32 year old? Because now your patient might have been only born with how many cusps of the aortic valve? Only two. How many should it normally have? Every single valve in the heart except the bicuspid has three cusps. So now the aortic valve only has two. That is congenital bicuspid disease resulting in early dystrophic calcification. This patient, 32 years of age, young, is having fatigue and tiredness upon exertion. If there is enough muscle build-up, a concentric hypertrophy of the left ventricular wall may result in angina maybe even chest pain upon exertion. Are you with me? Increased afterload. Tell me about that murmur. Where is it located? Where would you hear it? Second intercostal space point to it please, the right parasternal. 02:13 Where else might you hear it? That murmur, not the blood then may radiate up in the carotid. Is that clear? Increased pressure. So what are you going to do with all this? Take a look at physiology and with physio it is important that you take a look at the cardiac cycle. 02:33 It is important that we then compare this to pressure volume overload. Is this important? Yes and you know as well as I do as to how often that is asked on every single level of medical education. There are three main causes. Senile calcification. 02:49 So who is this patient? Not 32 year old probably would not take kindly to the fact that he or she is going to be referred to as being senile. Next, so senile would have to be someone who is 70-some. As we get older, our tissues, unfortunately, do get tired, old, damaged and may result in what kind of calcification? Senile dystrophic calcification. What is our topic? Aortic stenosis. 03:15 That would be the most common cause obviously. Can we prevent age from taking place? Not that I know unless you're Johnny Depp from Pirates of the Caribbean and he was looking for fountain of youth, you know his entire life got old in the process though, even he was not successful. Incidents increases with advancing age obviously. What is happening? The aortic valve was becoming damaged. How many cusps does this patient have? Three, which is getting old, damaged. Calcification, this is the 32 year old that I have been referring to a couple of times now. Congenital bicuspid aortic valve. Now what I do want you to pay attention to is don't just take a look at congenital and give it a generic name. What kind of congenital, or maybe the Down syndrome? Is that congenital? I believe so. What about Turner syndrome, XO? Would you have bicuspid? Of course these are congenital conditions. So any congenital anomaly might then also give rise to a bicuspid aortic valve and now prone to what? Dystrophic calcification at what age? Young and by young we are talking about 20s and 30s. Next, what else? In developing countries, not developed countries, the most common cause of aortic stenosis would be rheumatic heart disease. Is that clear? Now, what do you want to do with rheumatic heart disease? Be careful and the reason I say that is number 1, couple of ways in which your patient may develop this. We will talk about in greater detail and obviously hit upon this in microbiology. And you have a child that might have pharyngitis and that pharyngitis was caused by group A streptococci pyogenes and the pharyngitis was not properly treated and two to four weeks later ended up developing issues in the heart. So we have rheumatic fever, part of this might have been endocarditis. Or maybe it was impetigo. Impetigo could be caused by staph, but in this case streptococci pyogenes and may give rise to heart. Not so much. We will talk about that in more being with post-streptococcal, but at this point what I want to firmly or plant a seed in your head is the fact that streptococci infections do not only limited to pharyngitis. 05:35 It could also involve the skin, but each one of those would be giving rise to different types of diseases. So here we go. With rheumatic heart disease, if it is early on and damage to the valve. Listen to what I'm saying, early is the operative ward, then it would be a regurgitative issue. What is my topic? Stenosis. What do you think stenosis might mean in a rheumatic heart disease patient? It just caused damage. At some point in time, don't you think that repair process is kicking in. Of course it is. What does the repair process mean to you? Collagen coming in, deposition of fibrosis. So what does fibrosis mean to you? Hardening. Is that clear? Do not memorize this. So when you talk about rheumatic heart disease, 95 percent of your patients will have issues with the left-sided heart valves. "Dr. Raj, what about the right side?" Of course the right side could be involved with a measly five percent. So do you want to spend time on things that are uncommon? Why would you want to do that? Why would you want to make your life more difficult? So 95 percent of time, it would be the left side. On the left side, it would be aortic and mitral. 06:46 So those are the valves that will be affected early on it will be regurged. Our topic here is stenosis. Where is your patient coming from? Developing countries. What if there was a developed country? Congenital bicuspid or older 70-some, what kind? See now. Are you putting things together or are you creating differentials based on the history and demographics of your patient? Here with calcification, nice little cartoons, then differentiate between a normal and then you find calcification. How many cusps do you see here? One, two, three. 07:24 So it was normal and how old was this patient presenting with aortic stenosis and dystrophic calcification? Old, has to be senile. Three cusps. What if you only find two cusps? Then it will be young patient. Guaranteed. Is that clear? Here you only have two cusps. Do you see them? This is the aortic valve. This is not the bicuspid. That is the problem and so therefore at the age of 30-some ends up developing dystrophic calcification, aortic stenosis and let us go one step further. How does the left ventricle going to respond please? Hypertrophy and the left ventricle is lifting weights and what are the weights? The aortic stenosis. What is it going to do? Undergoes hypertrophy. What kind? Concentric hypertrophy. Let us go one step further. If that left ventricular wall becomes thickened, conceptualize this. What is the size of the chamber, please? Reduced. 08:21 When you have reduced size of the chamber because of increased thickness of the left ventricular wall, you cannot accommodate for more blood to come in. Is that a diastolic or systolic dysfunction? It is a diastolic dysfunction. In fact, clinically speaking, there is something called heart failure with preservation of your ejection fraction. HF heart failure. Preservation P. EF ejection fraction. So you can actually have heart failure with aortic stenosis early on, ejection fraction is normal. It still would be around 55 percent. 08:53 Is that clear? I will talk more about that later. You have discussed that in physio, but it is important that you bring it into play now.
About the Lecture
The lecture Aortic Stenosis: Pathogenesis by Carlo Raj, MD is from the course Valvular Heart Disease: Basic Principles with Carlo Raj.
Included Quiz Questions
What is the most common cause of aortic stenosis in older adults (> age 65) in the US?
- Calcific disease
- Coronary atherosclerosis
- Rheumatic fever
- Bicuspid valve
- Hypertension
Which of the following is the most likely cause of aortic stenosis in a 58-year-old man that immigrated to the United States from a developing country in Asia?
- Rheumatic heart disease
- Bicuspid valve
- Calcific disease or a trileaflet valve
- Atherosclerosis
- Hypertension
What type of pathological changes are seen in the left ventricle in a patient with aortic stenosis?
- Concentric hypertrophy and diastolic dysfunction
- Concentric hypertrophy and systolic dysfunction
- Eccentric hypertrophy and diastolic dysfunction
- Eccentric hypertrophy and systolic dysfunction
- Concentric atrophy and diastolic dysfunction
What is the most likely cause of heart failure in patients with aortic stenosis?
- Reduced chamber size of the left ventricle
- Increased chamber size of the left ventricle
- Reduced chamber size of the right ventricle
- Increased chamber size of the right ventricle
- Stenosis of the atrioventricular valves
Author of lecture Aortic Stenosis: Pathogenesis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
4 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Wonderful faculty Dr Carlo Raj. He has a unique style of Teaching which gives us the full Concept and a complete grip on the Topic. Makes difficult topics Easy to Learn.
LOL. That was a hilarious presentation of a serious topic. I enjoyed it a lot.
The most SUPER !!AWESOME!!AMAZING!!STUNNING lecture that I have seen in my whole life as a medical student. DR Carlo Raj has passion and intellectual ability to deliver His lectures in a manner that I have never witnessed before with any other lecturers. combining all the important physio points with path.I wish i could explain how happy I was jumping in my room after this lecture. Amazing! you are always my my hero Dr. Carlo. How I wish one day I could just have a handshake with you. May Allah bless , you and your family AMEEN!!. I would recommend this to all the international medical students preparing for the USMLE exam.
1 customer review without text
1 user review without text
