Playlist
Show Playlist
Hide Playlist
Hypertrophic Pyloric Stenosis: Examination

-
Slides Hypertrophic pyloric stenosis Special Surgery.pdf
-
Download Lecture Overview
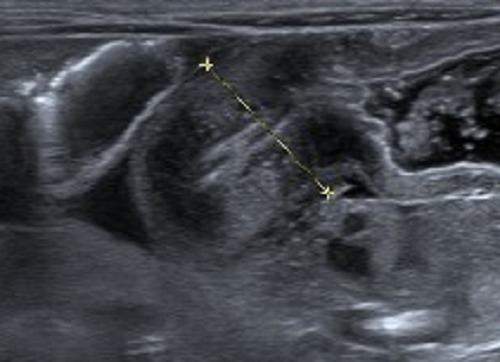
00:01 How do babies present? Classically, they vomit postprandially. 00:06 The emesis is usually non-bilious. 00:09 And the emesis is described classically as projectile. 00:14 This makes anatomic sense. 00:16 As a pyloric channel becomes stenotic, gastric content has nowhere to go. 00:21 It’s non-bilious because it does not have the opportunity to mix with bilious content in the duodenum. 00:27 Projectile, because as a stomach gets more and more distended, it's got a closed channel by the pylorus. 00:33 The only way the patient can drain gastric content is by forceful vomiting. 00:40 One important thing to notice is how the child is always hungry after vomiting and wants to feed again, a sign called the hungry vomiter. 00:49 On physical examination, we oftentimes find an olive mass in the upper quadrant of the abdomen. 00:55 Because babies have relatively thin abdominal walls, this is easier to appreciate. 01:00 On the left side of the screen is a palpation of the abdomen, finding this olive mass. 01:06 And on the right side of the screen is an ultrasound. 01:09 We’ll get to that in a second. 01:11 Aside from a baby who may have projectile vomiting, they also have sunken fontanelles. 01:20 What does that mean? As you’ll remember, the skull has not completely fused in an infant. 01:25 And one of the first signs of dehydration is sunken fontanelles. 01:29 A lethargic baby. 01:33 This, obviously, is not specific to hypertrophic pyloric stenosis. 01:37 As you'll recall from many other pediatric modules, a lethargic baby or one that has failure to thrive is an ill baby. 01:45 There are some important findings on chemistry with patients with non-bilious projectile vomiting, such as in hypertrophic pyloric stenosis. 01:54 Low sodium, low chloride, and low bicarb. 01:59 The CBC may actually be completely normal. 02:02 Next, let's move to an ultrasound imaging. 02:06 Ultrasound imaging is first-line therapy. 02:08 Again, it doesn't introduce any radiation to the baby. 02:12 An ultrasound is particularly useful for pyloric channel stenosis. 02:16 Here in this image, you notice two white dots on the image. 02:20 It’s actually measuring the thickness of the channel. 02:23 Not only is the thickness important, the length of the channel is also important.
About the Lecture
The lecture Hypertrophic Pyloric Stenosis: Examination by Kevin Pei, MD is from the course Special Surgery.
Included Quiz Questions
How would you describe the vomitous seen in hypertrophic pyloric stenosis?
- Non-bilious
- Bloody
- Bilious
- Pre-prandial
- Non-projectile
Which of the following findings are seen in cases of hypertrophic pyloric stenosis?
- Olive mass in the upper abdomen
- Irregular mass below the right rib cage
- Spongy-feeling mass on both sides of the flank
- Tenderness at McBurney's point
- Tender, irregularly shaped mass in the right upper quadrant
Author of lecture Hypertrophic Pyloric Stenosis: Examination

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Explained in a way to understand very well for all . Presentation is good
