Playlist
Show Playlist
Hide Playlist
Hypo- and Hyperglycemia: Diabetic States





-
Emergency Medicine Bord Hypo and Hyperglycemia.pdf
-
Download Lecture Overview
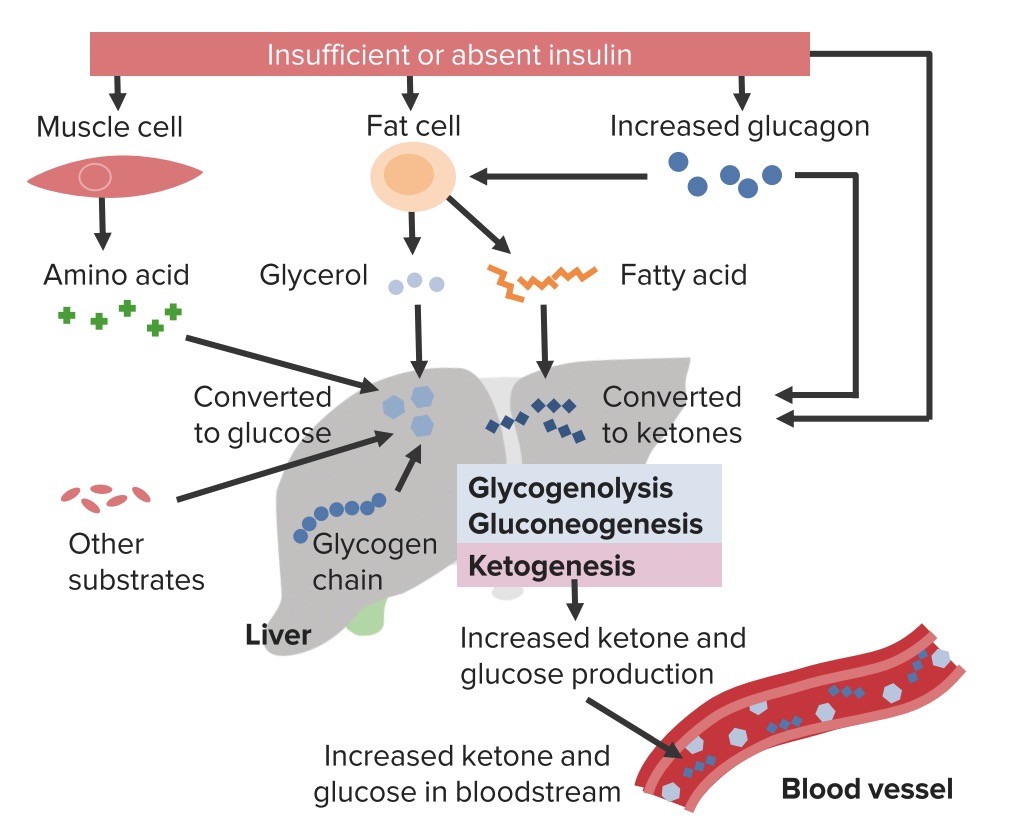
00:01 Hi. 00:01 Were gonna be talking about hypo and hyperglycemia, and how to manage these conditions in the Emergency Department. 00:10 We’re gonna start off by reviewing normal glucose metabolism. 00:14 Normal fasting glucose levels in plasma are 70 to 99 mg/deciliter. 00:19 Impaired fasting glucose (prediabetes) levels are 100 to 125 mg/deciliter. 00:26 Diabetes can be diagnosed if fasting glucose levels are more than 125 mg/deciliter on at least two occasions. 00:34 In the emergency department, a glucose level less than 70 mg/dL needs further evaluation and treatment; if the level is greater than 150 mg/dL, further evaluation is needed, with possible treatment. 00:49 It’s important to remember that glucose is the primary energy source for our bodies. 00:53 So we wanna make sure that we're keeping it within this appropriate range. 00:59 Now, where does glucose come from? So glucose comes from the foods that we eat. 01:04 When we eat foods, our intestines absorbs some of the glucose. 01:08 Glucose also comes from gluconeogenesis. 01:11 And gluconeogenesis is basically glucose that is made from precursors, such as lactate, pyruvate, and amino acids. 01:20 Glucose for our body also comes from something called glycogenolysis. 01:25 What this basically means is these are glucose stores that are getting broken down. 01:30 Primarily, the glycogen from our liver that's stored there for times that were not able to eat gets broken down by the body and gets released into the bloodstream. 01:42 We have few primary regulatory hormones for glucose within our body. 01:46 So one of them is insulin and what insulin does, is it leads to glucose storage. 01:51 So basically, after that insulin — after the glucose that we eat gets absorbed from our body, insulin is secreted by pancreas or released from the pancreas, and what that causes our body to do is it causes the body to store some of that glucose. 02:07 Some of it is used immediately by our bodies, but some of it gets stored in the liver in the form of glycogen. 02:14 The other primary regulatory hormone is glucagon. 02:18 And glucagon leads to glucose release. 02:20 So while insulin causes the pancreas or causes the body to store the glucose. 02:26 So they put it in storage and package it up. 02:29 Glucagon leads to breaking down of the glycogen in our bodies to release glucose. 02:35 Now, these are both released in different times, like I mentioned, insulin is released after one eats. 02:42 Glucagon is released in time periods that you have longer times between meals or your body doesn’t have enough glucose available to it, it will signal the body to release that glucose. 02:55 You know, there are couple different diabetic states, we’re gonna start here by talking about hyperglycemia. 03:01 When we’re thinking about hyperglycemia, we divide it into two different diabetic categories. 03:07 So the first is type one. 03:09 So what is type one diabetes? Type one is characterized by the acute absence of insulin. 03:15 So this is our body not making insulin anymore. 03:19 These people are prone to ketosis. 03:21 We’re gonna talk about diabetic ketoacidosis. 03:24 And what these basically means, is that our bodies, when they don’t have insulin, will go ahead and break down other products which will lead to ketone body formation. 03:35 It's generally caused by autoimmune destruction of beta-cells in the pancreas. 03:39 So the beta-cells are the cells of the pancreas that release the insulin, and our body is essentially responding to those and destroying them. 03:49 These patients require parenteral insulin. 03:52 These patients are gonna need to be maintained on insulin, because the key pathophysiologic process here is the fact that there is no insulin, your body is not making it. 04:03 Now, this is distinguished from type two. 04:05 Type two patients may remain asymptomatic for a long period of time. 04:10 So they may not necessarily recognize that they're in a diabetic state. 04:16 For these patients, insulin levels may actually be low, normal or high, and the key tenant here is that they have an element of insulin resistance. 04:26 So even if the insulin levels are normal or elevated, our tissues in the tissues in the body aren't responding to that. 04:33 Now, ketosis here is rare. 04:35 So these patients will more likely get HHS rather than getting diabetic ketoacidosis. 04:43 There’s also an association with obesity for these patients as well as elevated triglyceride levels. 04:49 Now, the rates of diabetic patients are on the rise. 04:52 Nine percent of Americans have diabetes, and 12% of adults greater than 20 years old have diabetes as well, and these numbers are only increasing. The rates of childs with obesity are increasing and this is a major public health crisis for the United States. 05:11 There’s also lot of morbidity and mortality associated with diabetes. 05:16 So diabetes predisposes patients to cardiovascular disease, to stroke, to renal failure, to problems with their vision. 05:24 And all of these has major implications for patients as they get older and as they develop these conditions. 05:33 I always talk with patients who come in with elevated blood sugar about these complications, 'cause some of them such as renal failure, and eyesight can potentially be prevented or staved off by good glucose control. 05:47 I tell people, if you wanna not go on dialysis, if you wanna be able to see, you need to make sure that you are controlling your glucose well. 05:57 Now, the presenting symptoms and clinical features of each of these conditions. 06:02 So for type one diabetes this is generally gonna be a lean patient. 06:06 This is gonna be a patients who’s gonna be on the thinner side. 06:09 Patients generally are younger, less than 40 years old, and generally, the pediatric patients who present with hyperglycemia and diabetes for the most part, historically have fallen into this category. 06:21 However, now that we have increasing rates of childs with obesity, it’s possible that the patients may commonly form — may more often now fall into that type two category as kids. 06:35 There’s also the classic polys, so polydipsia, polyphagia, polyuria and weight loss. 06:41 So what these polys mean are that your patient is gonna be drinking more, eating more and urinating more. 06:48 Generally, it’s a rapid development of symptoms. 06:50 So patients are well and then all of a sudden over a period of days or weeks, they start to feel really lousy. 06:57 This decompensates to DKA. 07:00 So when patients don’t take their medication, when their body is under stress, diabetic ketoacidosis can develop. 07:07 Type two diabetes historically and classicaly are thought to be most likely obese patients. 07:13 It’s important to remember though that not everyone who has this is overweight or obese, and 20% of the patients are not. 07:21 Generally again, older people but with increasing rates of childs with obesity, this may present younger and younger for patients. 07:30 It’s also more of a gradual symptom onset. 07:32 So patients are gonna have potentially similar symptoms to the type one diabetic developing. So the polydipsia, the polyuria, but it’s gonna occur more gradually rather than taking that shorter period of time. 07:44 These decompensates to HHS, which is a hyperglycemic hyperosmolar syndrome.
About the Lecture
The lecture Hypo- and Hyperglycemia: Diabetic States by Sharon Bord, MD is from the course Endocrine and Electrolyte Emergencies. It contains the following chapters:
- Hypo- and Hyperglycemia
- Diabetic States
Included Quiz Questions
What hormone regulates the storage of glucose?
- Insulin
- Glucagon
- Leptin
- Ghrelin
- Cortisol
What hormone regulates the release of glucose into the blood stream?
- Glucagon
- Insulin
- Ghrelin
- Leptin
- Cortisol
Which of the following does not describe Type 1 diabetes?
- Associated with obesity
- Acute absence of insulin
- Prone to ketosis
- Autoimmune destruction of beta-cells in the pancreas
- Requires parenteral insulin
Author of lecture Hypo- and Hyperglycemia: Diabetic States

Sharon Bord, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
