Playlist
Show Playlist
Hide Playlist
Fetal circulation and Transition to Mature Circulation

-
Slides 06-34 Fetal circulation and the transition to mature circulation.pdf
-
Download Lecture Overview
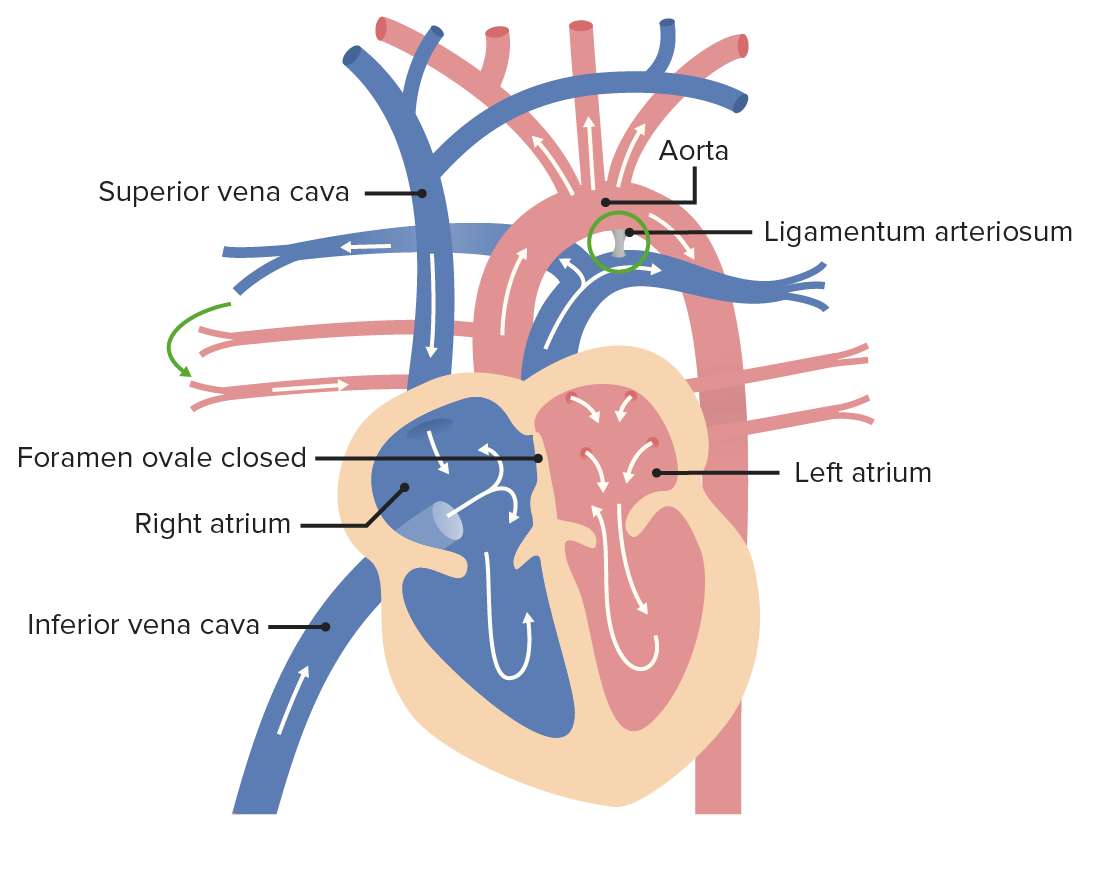
00:01 Welcome to the last talk on development of the vascular system and we're gonna track how changes in the fetal circulation occur the moment we take our first breath and we transition almost entirely all at once to the mature circulation. 00:13 And I've got some good news. 00:14 If you have been suffering through all the prior talks on heart development, vascular development, venous development, this talk is the payoff. 00:23 This is where it actually all comes together and we get to see that amazing moment when the blood transitions from one set of functional circuitry to a completely different but equally functional set of flow. 00:36 So we're gonna start by reviewing how the venous drainage and embryonic blood supply work overall and what happens that moment we take our first breath. 00:46 Now, recall that in the womb, we're getting all of our oxygen through the placenta. 00:52 The placenta is bringing blood into the fetal body through the umbilical vein. 00:57 The umbilical vein passes though the liver but doesn't lose much of its blood to the liver because a large channel, the ductus venosus, carries it to the inferior vena cava. 01:07 Now, in the inferior vena cava, it does mix with venous blood that's returning from the embryos, organs, and lower limbs. 01:14 So even the best oxygenated blood that the fetus is receiving is still slightly deoxygenated compared to what we'd expect. 01:23 Now, that blood is carried through the inferior vena cava to the right atrium and because of the way it enters that right atrium, it's going to hit the atrial septum in such a way that it pushes the valve of the foramen ovale out of the way and most of that oxygenated blood moves straight from the right atrium, into the left atrium. 01:43 Once it's there, it's going to then move to the left ventricle and be pumped out to the aorta. 01:50 Now, you may note that some blood coming from the lungs and the pulmonary veins is also entering the left ventricle but there's not much. 01:58 And so the majority of blood being pumped by the left ventricle out to the system is still oxygenated coming more or less directly from the placenta. 02:07 And that's how the organs of the body are getting blood that allows them to develop. 02:12 That blood's carried throughout the body but one of the things that can happen as it goes is it can travel through the iliac arteries and thereafter into the umbilical arteries, that travel back up the body wall, out through the umbilical cord, and to the placenta. 02:29 And that's how the placenta has continual replenishment of blood supply. 02:34 Deoxygenated blood coming from the body goes to the placenta, passes back into the body through the umbilical vein to get to the heart and be pumped elsewhere. 02:43 So all of that's happening and allows the fetus to develop. 02:47 What's going to happen at this point is that we're gonna get ready for the transition but before we do that, I want you to note that we still have venous return coming into the superior vena cava, inferior vena cava, and coming into the right atrium. 03:01 Now, the superior vena cava is coming into the right atrium at such an angle that it's preferentially directed into the right ventricle and then, gets pumped into the pulmonary trunk and out to the lungs. 03:12 But you'll notice that the pulmonary trunk and pulmonary veins are shown here relatively small and that's on purpose. 03:20 It's because there's not a whole lot of blood that's travelling to the lungs. 03:24 In uteral, we're surrounded by amniotic fluid and in fact, we spend a lot of time in that amniotic fluid breathing it in. 03:32 So we're pulling fluid into our lungs and getting a good workout for our respiratory muscles the whole time we're developing. 03:40 So the lungs are not full of air because there's no air to be had in the womb, they're full of fluid. 03:44 Fluid is high pressure. 03:47 So the blood in the pulmonary arteries is trying to get to the lungs but because of the pressure there, it has a tough time. 03:54 Fortunately, we have an outlet. 03:57 We have the ductus arteriosus connecting the pulmonary trunk to the aorta. 04:02 And the blood that can't push its way into the lungs is gonna spill out through the ductus arteriosus, into the descending aorta, and thereafter, the blood going to the organs, the lower limbs, and thankfully, the umbilical arteries is going to be relatively poorly oxygenated. 04:18 Now, let's say birth just happened. 04:22 We've taken our first breath. 04:24 The lungs have cleared a lot of that amniotic fluid and are now full of air. 04:29 What's gonna happen? Well, at the same time we're taking that first breath of air, we're losing our placental blood supply. 04:37 We're basically having the placenta get clamped and blood to and from it is no longer going to be present. 04:44 So the umbilical vein is going to cease to have blood flow through it and will eventually just become a ligamentous structure that's going to travel up the anterior body wall. 04:54 It's called the round ligament of the liver or ligamentum teres hepatis and the ductus venosus that traveled through the liver is also going to become fibrous becoming the ligamentum venosum. 05:06 Now, at this point, the only blood travelling in the inferior vena cava is venous blood returning from the lower limbs and the organs. 05:15 It's gonna make it to the right atrium. 05:17 Now, instead of pushing through the foramen ovale, it's gonna stay on the right side. 05:23 And that's partially because there's less blood in there. 05:26 There's no longer any placental blood supply coming in, so there's less pressure. 05:29 But because we've taken that first breath, all of a sudden, the pressure in the lungs has dropped tremendously. 05:37 More blood starts travelling to the lungs and not surprisingly, more blood starts returning from the lungs and that blood is going to return into the left atrium. 05:48 And the left atrium is going to have so much pressure in it that it slaps the valve of the foramen ovale shut and winds up completely separating the right atrium from the left atrium. 06:00 And now, we have a situation where the right side of the heart is almost exclusively deoxygenated blood and the left side is almost exclusively oxygenated blood. 06:10 And that very well richly oxygenated blood is pumped from the left atrium to the left ventricle, to the aorta and then, throughout the body. 06:19 And you can see here colored in red, we've got good profusion of the organs, lower limbs, just as the umbilical vein became fibrous, the umbilical arteries no longer have anywhere to go. 06:31 So they give off some branches to the bladder called the superior vesicle arteries but the remnant of them that would've gone to the placenta and umbilicus, are going to become fibrous and are thereafter called the medical umbilical ligaments. 06:45 The last major transition that occurs just after birth is that we no longer need the ductus arteriosus to take blood from the pulmonary trunk into the aorta. 06:57 The lungs are now getting a lot of blood and returning a lot of blood. 07:00 So if we had that shunt still present, it would no longer be a right to left shunt of pulmonary to systemic, it would turn into a left to right shunt as high pressure blood in the aorta pushes its way into the pulmonary circuitry and we don't really want that. 07:18 The good news is there's smooth muscle in the wall of the ductus arteriosus and when it senses an increased amount of oxygen within the blood, it will constrict and narrow, and narrow, and narrow, and become a fibrous structure called the ligamentum arteriosum. 07:35 So one thing to remember is that the ducts always end in 'us?. 07:39 Ductus venosus, ductus arteriosus. 07:42 And the ligaments are always 'um?. 07:44 Ligamentum arteriosum, ligamentum venosum and so forth. 07:48 Now, the ductus arteriosus typically closes within a few days of birth and it's not a medical emergency if it's open immediately after birth. 08:00 It will be tracked to make sure it eventually does close up but a patent ductus arteriosus that stays in place is a problem because we don't want the blood in the aorta transitioning into the pulmonary circuit and mixing. 08:14 That left to right shunt will eventually cause problems and it will need to be repaired if it persists. 08:21 So it may close spontaneously but you may have to do it surgically if it's gonna be around for a while. 08:26 It's gonna cause hypertension inside the pulmonary circuitry and eventually, congestive heart failure as the right ventricle keeps trying to push against that additional pressure that's coming at it from above. 08:38 Now, the other thing about patent ductus arteriosus that's very important is that if you have other heart malformations, you may have to have a patent ductus arteriosus. 08:48 You might recall that a preductal coarctation of the aorta needs to have a ductus arteriosus present because otherwise, there's no way for a significant amount of blood of any kind to get to the lower limbs and the developing organs. 09:04 Thank you very much for your attention and I hope this has been enlightening.
About the Lecture
The lecture Fetal circulation and Transition to Mature Circulation by Peter Ward, PhD is from the course Development of Thoracic Region and Vasculature.
Included Quiz Questions
The oxygenated blood from the placenta is delivered to the fetus via what vessel?
- Umbilical vein
- Vitelline vein
- Umbilical artery
- Anterior cardinal vein
- Posterior cardinal vein
The oxygenated blood that enters the right atrium from the inferior vena cava is shunted to the left atrium through what passageway?
- Foramen ovale
- Septum primum
- Ostium primum
- Fossa ovalis
- Foramen secundum
Blood that cannot surpass the high pressure of the fluid-filled lungs passes through what structure to reach the descending aorta?
- Ductus arteriosus
- Ductus venosus
- Sinus venosus
- Vitelline vein
- Umbilical artery
The deoxygenated blood returns to the placenta through what vessel?
- Umbilical artery
- Umbilical vein
- Vitelline artery
- Vitelline vein
- Ductus venosus
What is the remnant of the umbilical vein in adults?
- Ligamentum teres hepatis
- Ligamentum venosum
- Medial umbilical ligament
- Ligamentum arteriosum
- Median umbilical ligament
Which of the following vessels does NOT supply blood to the adult heart or the fetal heart?
- Pulmonary artery
- Superior vena cava
- Left anterior descending coronary artery
- Left circumflex coronary artery
- Pulmonary vein
Author of lecture Fetal circulation and Transition to Mature Circulation

Peter Ward, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
4 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Definitely decent videos. I love it deeply, and It helps me a lot. Woo. Dus goes us. Um go with um.
It felt like everything I learnt on the development of the heart came together, feels good
excellent & simple overview of the topic - He explain it in good way thanks a lot
I liked the way you explained the whole lecture in a simple way.
