Playlist
Show Playlist
Hide Playlist
Regurgitation and Clinical Consequences – Valvular Heart Disease

-
Slides Valvular Hypertensive Heart Disease.pdf
-
Download Lecture Overview
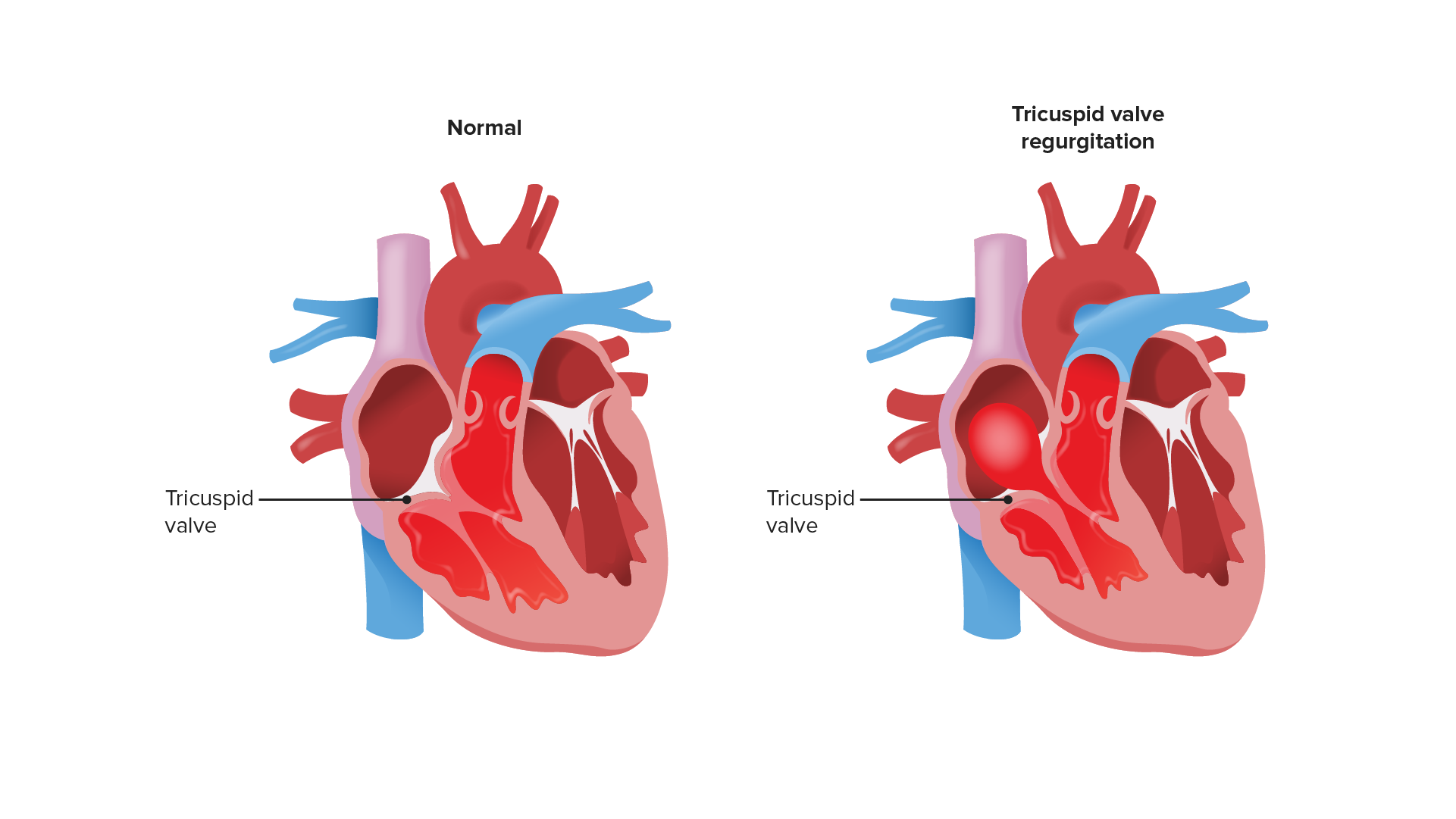
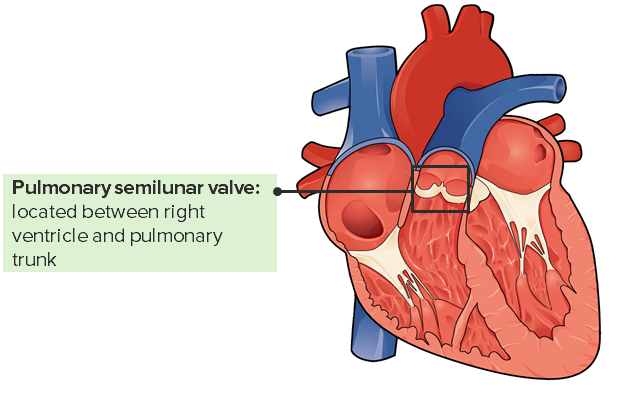
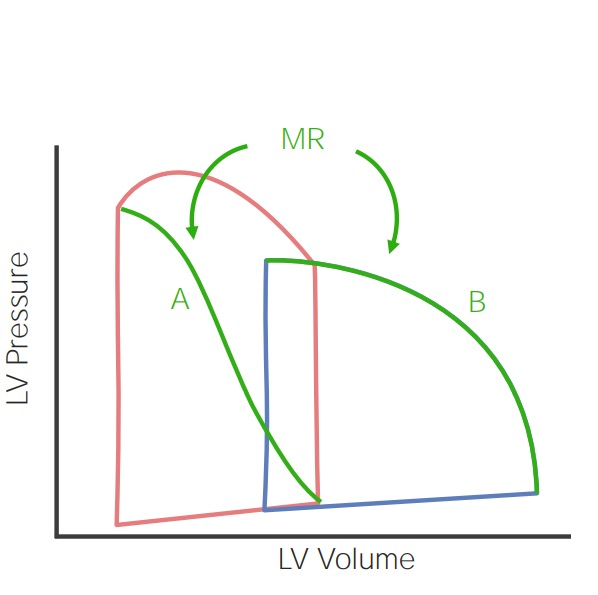
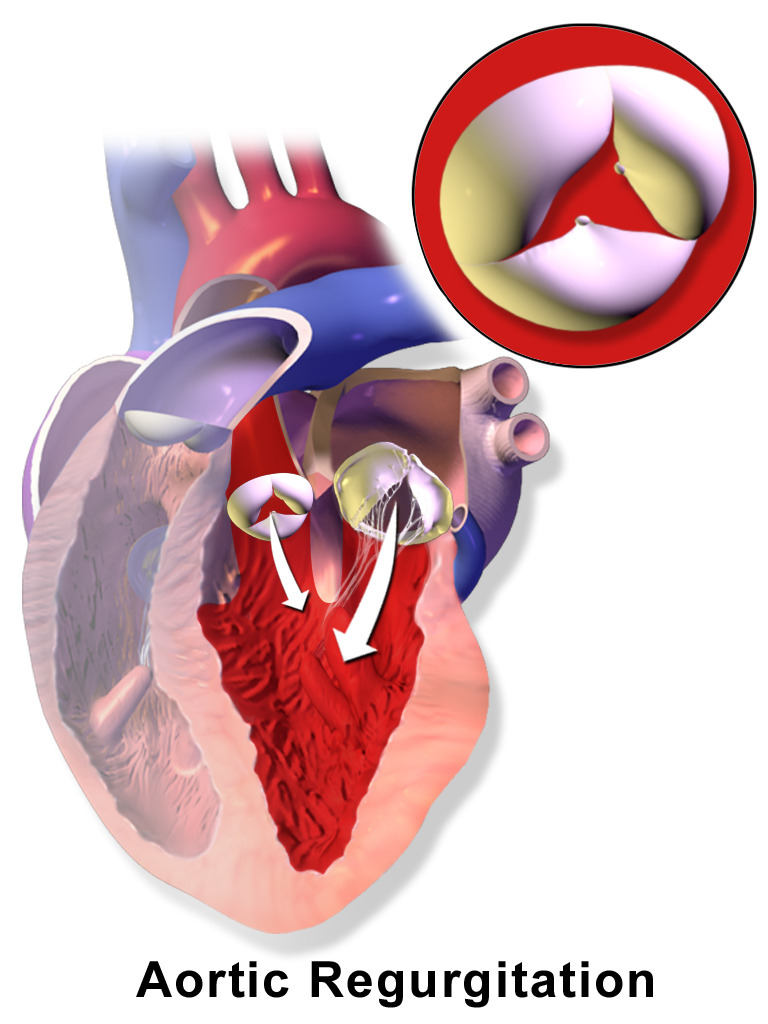
00:00 Welcome back. In this talk, we're going to cover valvular heart disease. 00:05 And there are a lot of different ways that we can have the heart valves affected, causing either stenosis or regurgitation. 00:16 And when the valves don't work to limit flow in one direction or another, then we have potential secondary complications that can be fairly significant. 00:26 This is just showing you the heart pumping. 00:30 It's a very vigorously pumping heart, just going from the left to the right on your screen. 00:36 We have blood that comes in the right atrium, goes across the tricuspid valve into the right ventricle, the right ventricle squeezes it out through the pulmonic valve, going to the lungs. 00:47 Blood returns oxygenated from the lungs to the left atrium. 00:51 And then, from the left atrium across the mitral valve, into the left ventricle which squeezes it out through the aortic valve. 00:58 We're going to talk about each of these valves and the pathologies that can occur with them. 01:03 And there are certain valves that are more predisposed to disease, such as the mitral valve. 01:07 Valves that are relatively uncommonly affected, the pulmonic valve. 01:12 And we'll talk about, again, insufficiency and stenosis. 01:16 So, stenosis, what is that? Well, it's basically the valve doesn't open completely. 01:22 It becomes stiff usually due to excess connective tissue or scarring. 01:28 And when that happens, as is shown here with aortic valve, you have a valve that doesn't open completely, and that impedes forward flow, giving you a jet stream going out, you see across the aortic valve into the aorta, but it also means that the left ventricle behind it has to work that much harder. 01:45 In insufficiency, the valve is incompetent. 01:49 Again, we're looking at the aortic valve, it's not closing appropriately. 01:52 So, when you have a filling during diastole, that valve should close. 01:57 Instead, the blood is regurgitating back from the aorta into the left ventricle. 02:03 This is not going to necessarily require the heart to squeeze harder, but there is going to be a volume overload. 02:10 We are basically dumping contents of the left ventricle recurrently back into the left ventricle. 02:17 And over time, that can also be a cause of heart failure. 02:20 Also, keep in mind that if you have insufficiency that's like this, we're not pumping all that blood out to the rest of the body. 02:26 So, you may have relative hypotension and malperfusion of all of the organs throughout the body. 02:32 Functional regurgitation can occur for a variety of reasons, and it can stem from, in this particular case, we're going to look at the mitral valve, so the atrial ventricular valve, the mitral valve, and the regurgitation can occur as a result of incompetence or defect in a number of support structures. 02:53 So, the annulus, the ring of fibrous connective tissue that holds the valve leaflets, needs to be competent. It can't be dilated. It can't be too tight. 03:04 It needs to maintain its normal circumference in order to keep the valve leaflets so that they can appropriately coapt, close against one another. 03:14 The valve leaflets need to be intact. If there's a hole in them, if the valve is destroyed, if the valve is too fibrotic, the valve won't close appropriately, and may become stenotic or regurgitant. 03:29 The chordae tendineae of the atrioventricular valves are also very important. 03:35 They connect the valve leaflets to the underlying papillary muscles, and they need to be of the appropriate length and tensile strength. 03:44 The papillary muscles connected to the left ventricular wall are also important. 03:49 They need to contract appropriately and relax appropriately to allow the valve to open and close respectively. 03:56 And the ventricular wall, the configuration, the geometry of that ventricular wall, has also got to be about right. Otherwise, as we'll see if the valve - if the ventricular wall dilates, then we pull those papillary muscles apart which pull on the chordae tendineae, and the valve leaflet won't close. So, the ventricular wall also makes a difference. 04:17 So, all of these structures are important for the function of the atrioventricular valves. 04:22 Now, we've been talking about the mitral valve in particular, but if you just shift over to the right, the tricuspid valve has all the same requirements in order for it to maintain its normal valvular structure and function. 04:37 Here's just an example of now where the chamber dilates. The left ventricle. 04:43 Everything else is fine. The annulus is fine, the leaflets are fine, the chordae is fine, the papillary muscles are actually okay, but the chamber now has a different geometry, and that dilation pulls the papillary muscles down and outward. 04:57 And now, the leaflets can't coapt. And so, that will lead to regurgitation. 05:02 It's a structurally normal valve but can't properly close. 05:07 So, things like ischemic heart disease can very easily cause mitral insufficiency. 05:14 And as we'll talk about when there's mitral insufficiency, blood is now going to be squeezed primarily through the low-pressure system, through the open valve, into the left atrium, and that pressure then translates back up into the lungs. 05:27 We have functional regurgitation with a completely normal valve in this case. 05:32 So, the clinical consequences clearly depend on which valve is involved. 05:38 And we can see that we're jumping around to the different ones, but tricuspid valve insufficiency has a different kind of consequence versus mitral insufficiency. 05:47 Tricuspid is going to affect the venous circulation systemically. 05:53 Mitral incompetency is going to affect the pulmonary venous circulation rather than the systemic. 05:59 Aortic stenosis versus pulmonic stenosis will have effects that you can, in your own mind, think through. 06:06 So, the nature of the valve or which valve is involved is important. 06:10 The degree of impairment, clearly, has an impact as well. 06:14 So, if you have severe stenosis such as that, then that's going to be much more of an effect than if it's a relatively minor calcification and stenosis for example. 06:25 And then, the tempo of the disease onset. 06:28 So, if it's very rapid, say, an infective endocarditis where you have a sudden destruction of the aortic valve, that's going to lead to acute massive rapidly fatal regurgitation. 06:38 However, if things go relatively slowly, such as mitral - rheumatic mitral disease, it's a slow degeneration, takes months to years, even decades, and for long periods of time, there will be adaptation of the underlying myocardium, and the other structures that will allow it to be well tolerated for extended periods until we reach, at some point, a tipping point where its symptomatology supervenes. 07:03 And then, it also depends on how well the heart can respond. 07:09 So, if you have a very good circulation and no atherosclerosis, you can tolerate valvular stenosis for longer. 07:16 You can have hypertrophy of the myocytes because you're providing adequate nutrition, adequate perfusion. 07:23 So, with pressure overload in a valvular stenosis case, you get concentric hypertrophy. 07:29 And if that goes slowly enough in a heart that has really good coronary arteries, you can compensate for a long, long period of time. 07:39 And conversely, if you have ischemic heart disease, you may not tolerate a valvular stenosis that well. 07:46 Valvular insufficiency, in another hand, gives you a volume overload which tends to give you what's called eccentric hypertrophy. 07:53 And the difference between concentric hypertrophy versus eccentric hypertrophy has to do with the alignment of the sarcomeres within the myocytes. 08:01 Concentric hypertrophy means that, in fact, you have increase in wall thickness. 08:08 Eccentric hypertrophy means you have increase in the diameter of the ventricle Both, over time, will lead to heart failure. 08:17 But it's important to note stenosis leading to pressure overload and valvular insufficiently leaving - leading to volume overload can have different kind of adaptation consequences for the myocardium.
About the Lecture
The lecture Regurgitation and Clinical Consequences – Valvular Heart Disease by Richard Mitchell, MD, PhD is from the course Valvular and Hypertensive Heart Disease.
Included Quiz Questions
How does blood flow across a valve change with valvular stenosis vs. valvular insufficiency?
- Stenosis impedes forward flow; insufficiency allows backward flow.
- Stenosis increases forward flow; insufficiency allows backward flow.
- Stenosis impedes forward flow; insufficiency impedes backward flow.
- Stenosis allows backward flow; insufficiency impedes forward flow.
- Stenosis impedes forward flow; insufficiency increases forward flow.
What is valvular functional regurgitation?
- Failure of coaptation of the valve leaflets without structural changes in the valve itself
- Valvular stenosis due to calcifications
- Valvular incompetence after surgery
- Failure of coaptation of the valve leaflets due to a defect in the valve itself
- Valvular incompetence due to infective endocarditis
How does the heart compensate for valvular stenosis vs. valvular insufficiency?
- Valvular stenosis >> pressure overload >> concentric hypertrophy Valvular insufficiency >> volume overload >> eccentric hypertrophy
- Valvular stenosis >> volume overload >> eccentric hypertrophy Valvular insufficiency >> pressure overload >> concentric hypertrophy
- Valvular stenosis >> pressure overload >> eccentric hypertrophy Valvular insufficiency >> volume overload >> concentric hypertrophy
- Valvular stenosis >> volume overload >> concentric hypertrophy Valvular insufficiency >> pressure overload >> eccentric hypertrophy
- Valvular stenosis >> pressure overload >> concentric hypertrophy Valvular insufficiency >> pressure overload >> concentric hypertrophy
Which of the following factors does NOT significantly impact the clinical course of valvular heart disease?
- Family history of heart disease
- Valve involvement
- Degree of valve impairment
- Speed of disease onset
- Quality of compensatory mechanisms
Author of lecture Regurgitation and Clinical Consequences – Valvular Heart Disease

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
fwqfqwf wqgqwg qwa fwqfqwf wqgqwg qwa fwqfqwf wqgqwg qwa fwqfqwf wqgqwg qwa fwqfqwf wqgqwg qwa
