Playlist
Show Playlist
Hide Playlist
Tension Pneumothorax

-
Emergency Medicine Pulmonary Trauma.pdf
-
Download Lecture Overview
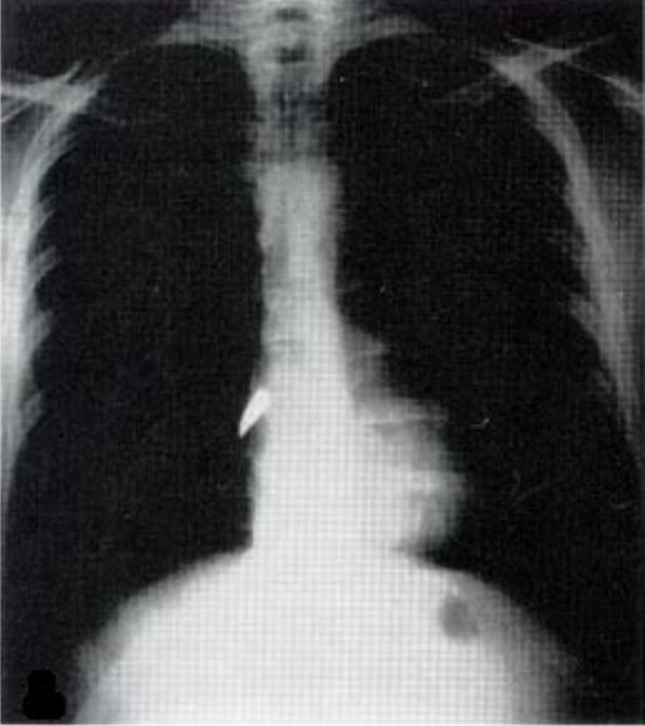
00:01 So let’s start off with tension pneumothorax which is probably the most common and the most serious of the pulmonary life threats. 00:08 How does a tension pneumothorax work? Well, very simply, a pneumothorax occurs when air enters the pleural cavity. 00:15 In trauma, this is typically happening because of direct injury to the lung. 00:19 So if you have a stab wound to the chest, you penetrate the lung, air leaks out of the lung parenchyma into the pleural space. 00:27 In blunt trauma, it’s often rib fractures that will penetrate the lung, causing development of a pneumothorax. 00:33 A tension pneumothorax is a special subtype of pneumothorax which occurs when you have a one-way valve effect in the pleural space. 00:43 So basically, what happens in a tension pneumo is during inspiration, the patient is able to suck air through the trachea, through the lung, and out into the pleural space, but then during expiration, that one way valve slams shut and the air that entered the pleural space is unable to get back out. 01:03 So what happens is with each and every breath, the patient pulls more, and more, and more, and more air into the pleural space which causes a large high pressure air collection. 01:16 So what are the complications of this? Well, one, your patient will almost invariably be hypoxic because the tension pneumothorax will start off compressing the lung on the affected side but as it gets bigger, and bigger, and bigger, it’s gonna shift the mediastinum over to the contralateral side and cause compression on that side as well. 01:38 So you get significant hypoxia because the lungs are mechanically squished and unable to work properly. 01:45 You also get impaired cardiac filling. 01:47 So direct compression of the mediastinum from the large air collection is gonna compress the heart and prevent the heart from filling normally. 01:56 And lastly, you get impaired venous return. 01:59 So in normal physiology, blood comes back from the periphery into the central circulation because of negative intrathoracic pressure. 02:07 You can imagine if you have a large high pressure air collection in the chest, that your intrathoracic pressure is gonna be positive. 02:15 So now, you don’t have a pressure gradient that propels blood from the periphery back to the heart and this is gonna further impair your cardiac filling and your cardiac output. 02:26 So when we’re trying to diagnose a tension pneumothorax, we wanna listen for unilaterally absent breath sounds. 02:34 This is why the first step of our primary survey for breathing is bilateral auscultation of the lungs. 02:42 If breath sounds are absent on one side, you should strongly suspect a tension pneumothorax. 02:47 We also wanna look for evidence of respiratory distress. 02:50 Our patients with pneumothoraces are often working very, very hard to breathe because their chest is already hyper expanded with this big air collection. 03:01 So they have to work hard to pull air into that overinflated chest and they’ll have clinical distress on exam. 03:08 They’re almost invariably gonna be tachypnic for the same reason. 03:11 We already talked about why they would become hypoxic and then, as you can imagine, the trachea is gonna be deviated away from the lesion because this big expanding air collection is gonna push everything off to the other side. 03:28 So an important thing to remember about tension pneumothorax is it doesn’t just affect the lung. 03:33 In addition to respiratory impairment, our patients are gonna have shock. 03:37 So I already mentioned that you have impaired venous return. 03:41 You have mechanical compression of the heart. 03:43 This is gonna prevent normal cardiac output from taking place. 03:48 So these patients are gonna be tachycardic. 03:50 They may be hypotensive, and tension pneumothorax represents a form of obstructive shock. 03:56 So we wanna look not only for evidence of pulmonary compromise, but also for evidence of circulatory compromise in our patients with tension pneumo. 04:05 Now, tension pneumothorax is not usually a radiologic diagnosis. 04:11 Usually, this is something we diagnose clinically. 04:14 But if you do happen to get an x-ray, there are some characteristic findings that you’re gonna expect to see. 04:19 On this image, we have lines outlining the separation of the lung from the pleural space. 04:25 Now, this patient must have some underlying lung pathology because you can actually see that the lung tissue is tethered to the pleura in one location. 04:32 Maybe he has some old scarring in that region from a prior injury, hard to know. 04:37 But he’s got two regions of air where you don’t see any lung markings and those are denoted here and here. 04:46 So you can see the line demarcating the lung tissue from empty air space and you can actually see inside of the air collections that there aren’t any lung markings. 04:57 You also see inferior displacement of the diaphragm. 05:01 So on the patient’s right hand side, I’ve outlined the normal contour of the diagram, and on the left-hand side, you can see it’s pushed down much lower and that’s because this high pressure air collection is taking up a lot of room in the chest and actually displacing it inferiorly, and for the same reason, it’s displacing the mediastinum which is normally a left-sided structure, into the middle or right-hand side of the chest. 05:26 Now, you don’t wanna get this x-ray. 05:30 Tension pneumothorax is a clinical diagnosis. 05:33 Getting an x-ray of a patient with a suspected tension pneumo is only gonna delay your treatment for the patient and it’s not necessary. 05:41 So if you have a clear cut tension pneumo on clinical grounds, go ahead and treat it. 05:46 Don’t wait around for radiographic confirmation.
About the Lecture
The lecture Tension Pneumothorax by Julianna Jung, MD, FACEP is from the course Trauma (Emergency Medicine).
Included Quiz Questions
What is the cause of hypoxia in tension pneumothorax?
- Mechanical compression of both lungs
- Mechanical compression of the heart
- Increased intrathoracic pressure
- Impaired venous return
- Impaired cardiac filling
Which of the following radiologic findings does NOT suggest tension pneumothorax?
- Pleural thickening
- Line separating lung from pleural space
- Absent lung parenchymal markings lateral to the separating line
- Inferior displacement of the diaphragm
- Shifting of mediastinum to the contralateral side
Which of the following statements regarding tension pneumothorax is INCORRECT?
- Radiologic confirmation of tension pneumothorax is required prior to initiation of treatment.
- Pneumothorax occurs when air enters the pleural cavity.
- Absence of breath sounds on one side suggests tension pneumothorax.
- Patients with pneumothorax may also suffer from obstructive shock.
- Tension pneumothorax is mainly a clinical diagnosis.
Author of lecture Tension Pneumothorax

Julianna Jung, MD, FACEP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
