Playlist
Show Playlist
Hide Playlist
Primary vs. Specific Amyloidosis

-
Rheumatology II 03 Amyloidosis.pdf
-
Download Lecture Overview
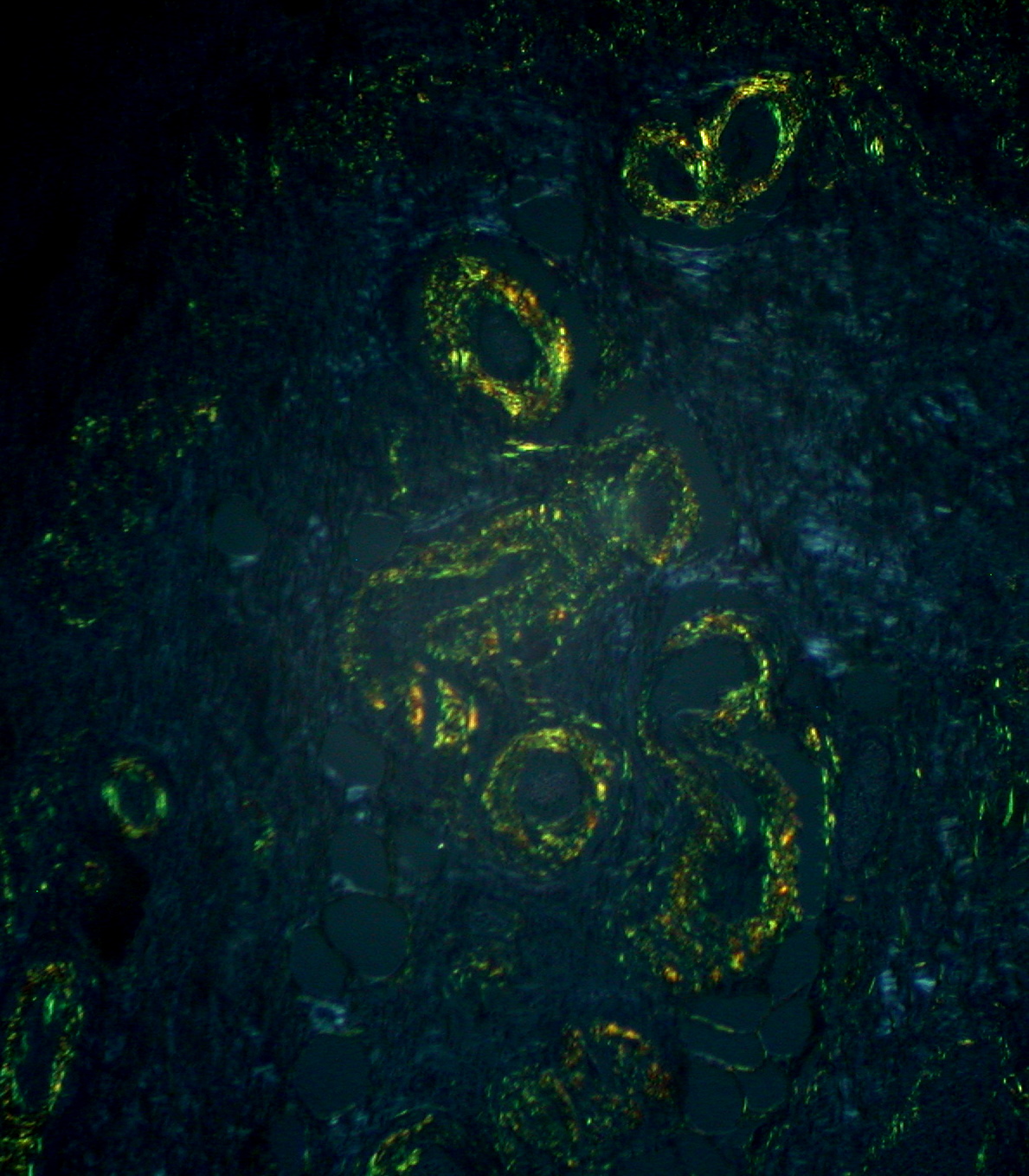
00:02 Here we shall have a discussion of an important topic called amyloidosis. 00:07 It’s short and sweet, to the point, and must understand as to how amyloidosis works in our body and how it manifests. Let’s begin. 00:17 So what is amyloidosis? Well at first, I’m going to walk you through the pathologic appearance of amyloid and how you must interpret it. 00:25 So the pathologic deposition of distinct protein in the extracellular space. 00:32 Appearance wise, if you were to take a look at it without proper staining, you see the areas that are rather thickened. 00:40 There are areas that you find to be thickened will be deposition of amyloid, we’ll just call this emorphous. 00:48 Now you suspect amyloid deposition, why? Well, I’ll walk you through some differentials later, including diabetes type 2, including transthyretin. 00:58 And at this point, you might be thinking about using Congo red stain, and when you find your Conga red stain then the color of your amyloid that you’d expect to find, would then be red or pink. 01:11 And then you’d do what’s known as a polarized microscopy, and when you do so, then you would find this to be apple-green birefringent. 01:19 The last time we had any discussion of birefringent was when we had our discussion of gout versus calcium pyrophosphate deposition. 01:27 Now what this picture is trying to tell us, is the fact that each one of these columns, are ways in which you may then accumulate commonly amyloid. 01:37 I say commonly because as we get older, we have senile amyloid that could then develop. 01:43 So what you’re seeing here on the left is that if there was a process that was a misfolded issue, and if there was a misfolded protein, such as for example protein Huntington in Huntington disease, or even let’s say CFTR, cystic fibrosis and such. 02:02 Then the type of amyloid that may develop is fibril. 02:06 And the production of abnormal amounts of protein, this might have occurred due to maybe disease processes or chronic inflammation. 02:15 Or let’s say that there is something like plasma cell dyscrasia, what does that mean? For example, you’ve heard of multiple myeloma, lytic bone lesions and so forth, right? And here, later on, we’ll talk about how you may then be using too much of the light chain, in particular light chain that produced a lot more would be kappa. 02:34 Anyhow, point is, you would then be producing your amyloid light protein. 02:38 Whereas if it is chronic type of inflammation, then you would call this amyloid protein or AA protein. 02:46 As we get older, there is every possibility that we may then just be accumulating normal transthyretin. ATTR stands for transthyretin and the A standing for amyloid. 02:57 These are, in general, different types of amyloids that you would then be forming on, well patients that you would see quite commonly for one reason or another or encounter in a clinical scenario, or clinical conference, what have you. 03:16 The primary amyloidosis that we will take a look at. 03:20 Let’s say that your patient did have lytic bone lesion, was a patient who was a male above the age of 50, and upon bone marrow aspirate ended up finding these plasma cells, and tons of them. 03:32 Well you might be thinking of myeloma as being one of your differentials. 03:36 You can take a look at the picture over to the right then you do remember the anatomy of an immunoglobulin, and immunoglobulin—I want you to focus on the following: You have a heavy chain and light chain, please identify the light chain. 03:49 The light chains in your plasma cell dyscrasia will start being increased in production. 03:57 If its multiple myeloma, if you remember, then it’d be either IgG or IgA, not IgM, and these light chains are then referred to as your amyloid light chains, and amyloid light chains may then deposit on the glomeruli, and when they do, you do the Congo red stain, even the fluorescents as such, and then you end up finding your apple-green birefringent, correct? And some of these light chains may then filter through, and when they do in the urine, you would then call this Bence Jones proteins as you’re quite familiar with, associated with plasma cell disorders. 04:29 Multiple myeloma would be one of them and Waldenstrom macroglobulinemia also known as lymphoplasmacytic lymphoma, then it’d be IgM or perhaps other B-cell lymphoproliferative disorders. 04:39 In general, light chains is what we’re looking at here, AL primary type. 04:47 If there’s deposition of amyloid fibrils, then this is then derived from your Ig lambda light chains is what you’re going to call this. 04:55 The amyloid light chains produced by plasma cells in multiple myeloma and Waldenstrom like we just said is our differentials. 05:05 The specific amyloidosis that you want to know, for sure, will be the following. 05:10 If a patient gets older and starts forgetting, obviously thinking about Alzheimer’s is a big problem. 05:17 With Alzheimer’s, you should be extremely familiar with amyloid beta protein. 05:22 Remember that each one of us are depositing tau, the taw would then be of course being your little spindles and such, and these are tangles that we deposit—all of us do, doesn’t correlate with the severity of the disease, but the more number of these tau tangles that we deposit, then you worry about amyloid aren’t you? Or in other words, Alzheimer’s. 05:45 Whereas now, if you’re talking about the amyloid, then you should be referring to the beta amyloid plaques. 05:51 The beta amyloid plaque is what we then call amyloid precursor protein (APP) Commit that to memory. 05:59 And then gene for precursor is on the protein of c21—keep that in mind—c21. 06:07 Since APP gene is located on chromosome 21, individuals with Down syndrome have an increased lifetime prevalence of Alzheimer’s disease. 06:20 If you have a patient who has a constellation of symptoms of maybe hypercalcemia, also has episodic hypertension, and in the urine you then find acid, and such, and then on a szintigramm of the thyroid you find a cold nodule. 06:36 Well what I gave you here was MEN 2a. 06:39 Again you have a parathyroidism I gave you chromocytoma, and here am giving you medullary cancer of the thyroid. 06:47 In medullary cancer of the thyroid, the type of amyloid deposit derived from calcitonin because of peripheral B cell producing too much calcitonin. 07:01 In type 2 diabetes, the type of amyloid derivative that you’re looking for is then called your well amyloid polypeptide or islet. 07:12 I, A—amyloid, P—poly, P—peptide. Often times you’ll see the abbreviation IAPP, sometimes referred to as being amylin. 07:27 Now please make sure that you’re quite familiar with knowing that type 2 diabetes mellitus the type that often times, the pathogenesis, being referred to with resistance—insulin resistance, where the receptors aren’t working. You with me? Especially as we get obese. 07:44 So therefore, or should I say, when I get obese —I can’t speak on your behalf is amylin or islet amyloid polypeptide is a particular amyloid derivative you want to keep in mind. 07:56 For amyloidosis, there is a huge variety of symptoms that can present with. 08:01 In the renal system, you can have asymptomatic proteinuria or nephrotic syndrome. 08:06 Looking on the cardiac system, there might be a heart failure, arrhythmia, or heart block. 08:12 In the GIT, it can result in hepatomegaly. 08:15 There are also neurological symptoms like peripheral neuropathy with CNS involvement such as vision or hearing loss is rare. 08:23 In the musculoskeletal system,it can result in pseudohypertrophy. 08:27 You can have a big amount of bleeding due to reduced factor 10 activity. 08:32 In the respiratory system, there might be persistent pulmonary effusions, nodules, or pulmonary hypertension. 08:39 And lastly on the skin, there might be subcutaneous nodules.
About the Lecture
The lecture Primary vs. Specific Amyloidosis by Carlo Raj, MD is from the course Muscle and Soft Tissue: Pathology.
Included Quiz Questions
A 75-year-old man with a 2-year history of loss of memory of recent events is brought to you because of increasing social disengagement and irritability over the past few months. What is the most likely diagnosis?
- Alzheimer disease
- Parkinson disease
- Multiple sclerosis
- Autism
- Creutzfeldt-Jakob disease
What type of extracellular deposits is characteristically seen in patients with Alzheimer disease?
- Amyloid beta
- Amyloid A protein
- Amyloid light chain
- Amylin
- Beta-2 microglobulin
Which of the following best describes Bence-Jones proteins?
- Immunoglobulin light chains found in the urine
- Immunoglobulin heavy chains found in the urine
- Immunoglobulin light chains found in the serum
- Immunoglobulin heavy chains found in the serum
- Immunoglobulins found in the urine
Which of the following peptides is deficient in patients with type 2 diabetes?
- Amylin
- Amyloid beta
- Serum amyloid A
- Calcitonin amyloid
- Beta-2 microglobulin
Author of lecture Primary vs. Specific Amyloidosis

Carlo Raj, MD
Customer reviews
4,5 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent lecture with the most important topics about the subject.
Great but more details need to be included in pathogeneses, please.
