Playlist
Show Playlist
Hide Playlist
Calcium Pyrophosphate Deposition Disease


-
Rheumatology I 01 Non-Autoimmune Arthritis.pdf
-
Download Lecture Overview
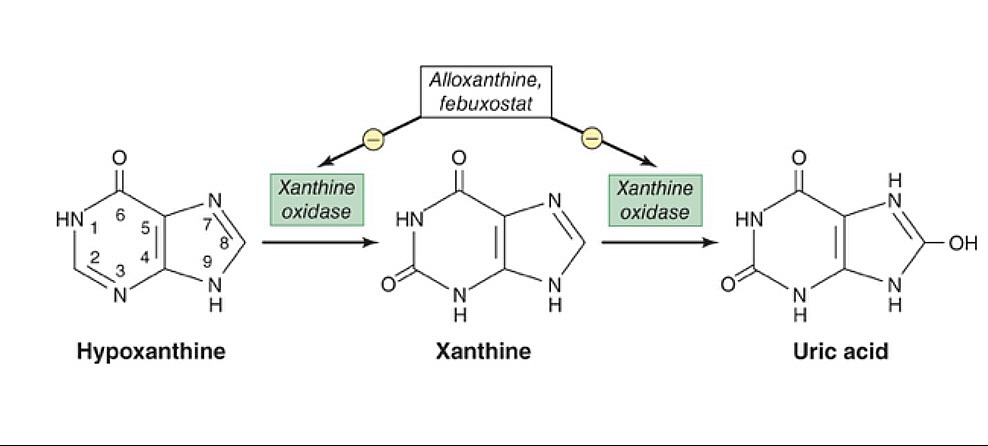
00:02 Now, that we've completed discussion of the gout, which by definition is accumulation of what? Uric acid. 00:08 Here we'll take a look at what's known as Calcium Pyrophosphate Deposition Disease, or CPPD. 00:15 You probably commonly in med school, and in your medical career have come across as being pseudogout. 00:20 I'll tell you why. I want you to stay away from that, because you need to understand the actual pathology. 00:27 So what is pseudogout? Oh, pseudogout is not the accumulation of uric acid. 00:32 So therefore, it's not gout. Pseudo, false. 00:35 So what is it? It's accumulation of calcium. Focus on that. 00:40 The full name is pyrophosphate. 00:42 And the full name is Calcium Pyrophosphate Deposition Disease. CPPD. Correct? I told you to focus on calcium. Why? Because presentation, especially when I give you the X-ray. 00:54 I'm going to show you, that there's going to be accumulation of calcium. 00:57 What color does calcium appear on X-ray? Opaque or loosened? Good, opaque. 01:05 So I'll show you something called chondrocalcinosis. 01:07 And while we go through this, obviously, you're going to compare this with the gout. 01:12 And you'll see how simple it is. 01:14 Pathogenesis, deposition of the calcium pyrophosphate. 01:19 Most commonly, where? Well, remember, in gout. 01:22 Where was the patient complaining of pain acute? In the big toe. Right? Watching the football game. "Oh, it hurts. Stop it." Yeah. Well, this is the large joints that you're looking for here in the pseudogout or CPPD. 01:37 Next, I told you to focus on calcium. 01:39 Chondro means cartilage. 01:40 So, in your joints, such as a knee and such. 01:44 You're [inaudible] going to accumulate calcium called chondrocalcinosis. 01:47 So, the meniscus of the knee, maybe the pubic symphysis and maybe the wrists. 01:52 These are large joints. 01:54 Now there are associations. 01:56 Metabolic disorders, such as: hyperparathyroidism. 02:01 What does that mean to you? Oh, increase calcium. There you go. 02:04 Maybe hemochromatosis association. Keep that in mind. 02:07 Could be hypothyroidism, hypomagnesemia, hypophosphatemia, and Wilson's disease, in other words, copper. 02:14 So there's important endocrine or electrolyte association that you want to keep in mind with deposition of CPPD. 02:24 Signs and symptoms. 02:25 Patient typically presents with acute symmetric arthritis. 02:30 What was it in gout? It was one toe, podagra, asymmetric, monoarticular. 02:37 These episodes are usually triggered by surgery, secondary to volume shifts, or even severe illness. 02:42 Keep that in mind. 02:45 And then, so we talked about how you could have pseudogout. 02:50 In other words, you know, the pain could be acute, it could be monoarticular. 02:54 However, over a long period of time, let's say that the knee has been involved, chronically. 03:00 But the presentation now, kind of feels like a wear and tear type of pain. 03:04 In other words, patient wakes up in the morning, it feels a little bit of stiffness, but less than one hour, maybe less than 30 minutes. 03:10 Seems like osteoarthritis, but it's not. 03:13 On X-ray you find calcium accumulating on the cartilage. 03:16 So therefore, in chronic CPPD, we then call this pseudo-osteoarthritis, or the pain might be greater than one hour. 03:27 Then this may seem like rheumatoid arthritis, you call this pseudo-rheumatoid arthritis. 03:34 We haven't talked about rheumatoid arthritis yet. 03:36 But this is all about depositing calcium pyrophosphate. 03:40 Acute, chronic. 03:42 So we have pseudogout, or we have pseudo-osteoarthritis, or pseudo-rheumatoid arthritis. 03:48 Keep that in mind for chronicity. 03:52 The calcium pyrophosphate now these are rhomboid. 03:56 What shaped were the gout crystals? Uric acid crystals? They were needle like, weren't they? What was the type of light that we use to identify the needles of gout? Polarized light. 04:09 Remind me again in gout, those uric acid crystals, were they negative or positive birefringent? In gout, it was negative birefringent. 04:19 If it was negative birefringent on polarized light, on parallel, was it yellow or blue? Yellow. 04:28 Completely different when we talked about CPPD. 04:30 Here we slightly positively birefringent, under polarized light. 04:39 Now, for you use parallel light, for positive, Guess what color that is? Blue. 04:48 So the biggest difference so far in polarized light has been with CPPD. 04:53 On parallel light, it will be positively birefringent, and he know it, because on parallel it will be blue. 05:00 If done parallel, it's yellow. That means it's negative. 05:04 Number one differential, gout. Is that understood? If not, make sure you repeat what I just mentioned. 05:10 Extremely important. 05:13 Next, we'll talk about calcium. 05:15 And once again here it is not uric acid, it's calcium. 05:19 So this made an appearance soft tissue as well. 05:21 What color is calcium? White on X-ray. In other words, opaque. 05:28 Management of CPPD acutely would be that similar to gout acute or we have anti-inflammatory drugs, such as NSAIDs. 05:39 You want to try to take care the prophylaxis? And prophylaxis usually will be with colchicine. 05:45 Remember associations that you could have including hyperparathyroidism, including hypothyroidism, hypomagnesemia, hemochromatosis, Wilson's, and such. 05:54 Associations that get underlying issue as well.
About the Lecture
The lecture Calcium Pyrophosphate Deposition Disease by Carlo Raj, MD is from the course Introduction and Non-Autoimmune Arthritis. It contains the following chapters:
- Introduction to Calcium Pyrophosphate Deposition Disease
- Diagnosis of CPPD
Included Quiz Questions
Which of the following conditions is LEAST likely to be associated with pseudogout (calcium pyrophosphate crystal deposition, CPPD)?
- Hyperthyroidism
- Hyperparathyroidism
- Hemochromatosis
- Hypothyroidism
- Hypophosphatasia
Which of the following best describes calcium pyrophosphate crystals?
- Rhomboid shaped and weakly positively birefringent under polarized light
- Needle shaped and positively birefringent under polarized light
- Needle shaped and negatively birefringent under polarized light
- Rhomboid shaped and negatively birefringent under polarized light
- Envelope shaped and positively birefringent under polarized light
What radiologic finding is often seen in calcium pyrophosphate deposition disease?
- Chondrocalcinosis
- Overhanging osteophytes
- Bone spurs
- Spondylosyndesis
- Subchondral sclerosis
Author of lecture Calcium Pyrophosphate Deposition Disease

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
