Playlist
Show Playlist
Hide Playlist
Primary Sclerosing Cholangitis

-
Slides GD liver disease.pdf
-
Download Lecture Overview
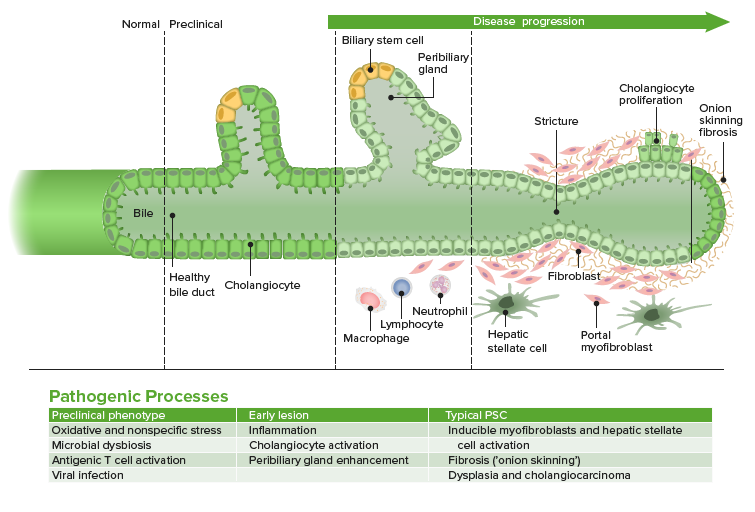
00:01 Primary Sclerosing Cholangitis. 00:04 Break up the name. 00:06 Primary beginning, arising by itself. 00:10 Sclerosing; narrowing of what? The bile duct. That is your topic. 00:15 Next. 00:16 What predictors of what we are going to discuss? It is an autoimmune disease for the most part. 00:22 Here, it is not AMA positive. 00:25 AMA positivity was found in Primary Biliary Cirrhosis. 00:30 Here, upon histology, I'd tell you about the onion skinning of the bile duct. 00:34 And with primary sclerosing cholangitis, If you narrow, one part of the bile duct, May I ask you a question, physiologically, If you take any tube, such a blood vessel or a duct or whatever, If you then narrow the distal end, what happened to the proximal end? Pathologically. 00:55 Dilation. 00:57 So you have narrowing. 00:59 Dilation, narrowing, dilation. 01:02 Doesn't it sound awfully a lot maybe perhaps Some of you might be wearing necklaces, beaded appearance. 01:10 When would you notice a beaded appearance with primary sclerosis cholangitis On an imaging study. 01:17 And we call that a cholengiogram. 01:20 Let's begin. 01:21 Inflammatory destruction of medium and large bile ducts; this affects however, young men. 01:27 More so. 01:29 90% are associated with ulcerated cholitis. 01:31 This is something that you will never find with primary biliary cirrhosis. 01:36 you will not find this. 01:37 90% percent is associated with ulcerated cholitis. 01:41 Where is that? Rectum. Alright? Remember, the rectum, continuous, ulcers, proximaly so, you move from the rectum up the descending colon and so forth. 01:54 And because of this, there is an increased risk of colorectal cancer CRC. 01:59 You see how different PSC is from PBC. 02:03 Spend a little time to make sure you are clear between the two diagnoses. 02:08 You cannot afford to get the two confused. 02:11 Along with colorectal cancer, and ulcerated colitis, there is a major major, association with cholengio carcinoma. 02:19 So, not only there could be cancer of the colon that might predisposed but my goodness, there is also predisposition of developing cancer of the gall bladder. 02:28 cholangio carcinoma. 02:30 You won't find this on Primary biliary cirrhosis. 02:33 Completely different. 02:36 Signs and symptoms here. 02:38 Let me ask you something. 02:40 If there is sclerosing and narrowing of the bile duct, after the liver, then what then happens? Well, from the liver, you conjugate bilirubin But you can't get past the bile duct because why? It is sclerosing. 02:57 So now, if you can't get past the bile duct into the gall bladder then, you're kind of backing up don't you? And if you back up enough, what is that called? We call this post hepatic jaundice. 03:12 Post hepatic jaundice. Let me ask you something else. 03:15 Did you poop this morning? You probably did. 03:18 If not maybe, whatever, that is your problem. 03:19 but anyhow, point being is so you went and passed stool this morning maybe. 03:24 And what color was your stool? Did you just take a look at it at the toilet? Hopefully it was brownish. right pigmented. 03:30 What contributes the pigmentation of that stool? Oh the bilirubin. 03:35 Right? bilirubin. 03:37 Not only does it give pigment to the stool, but it also gives you pigment to the urine. 03:42 If you can't past that block, in the bile duct. You can't get the bilirubin, into your intestine. 03:51 If you can't get the bilirubin to your intestine, Now, what color does your stool look like? Pale. 03:58 clay. 04:00 Right? Post hepatic jaundice. 04:02 Obstruction. I can't move my bilirubin further. 04:05 A post hepatic jaundice. In addition, you have pruritus-itching. 04:11 itching and yellowing of the skin, you should be thinking, hmm... 04:16 What system are you dealing with? At least know that you are dealing with the hepatic-biliary system. 04:20 and fatigue. 04:24 Diagnosis. 04:27 Do an MRCP or ERCP. 04:27 Endoscopic Retrograde Cholangio-Pancreatography This is then going to give an imaging what is this imaging going to give you? Remember, I told you, there will be narrowing or dilation narrowing, dilation, look for the description if they don't give you the image. 04:42 the description is called a beaded appearance. 04:45 If you then take the sclerosed area, and you do a cut section histology, what are you going to find? hyperplastic changes. 04:53 looks like onion-skinning. 04:55 Any time there is hyperplasia with a tube, it is called onion-skinning. 04:59 Ok, so don't get hanged up. There is no such thing as a buzzword. 05:02 I don't really like telling you that it is onion-skinning. 05:05 Because you know students immediately think: "Oh, it must be malignant hypertension Doctor Raj." No, it doesn't have to be. 05:11 Just because I said it is onion-skinning, I didn't tell you what kind of tube. 05:14 Here, I am telling you it is a bile duct. 05:17 There is no really effective therapy. 05:20 Maybe perhaps ursodiol. 05:22 Unfortunately, if you will allow for the disease to progress, then you're only option at this point once again will be, liver transplantation. 05:33 You'll notice here, on your left, is PSC - Primary Sclerosing Cholangitis. 05:39 What's shown here is extremely opaque, it is going to be opacity but then, I want you to go and start moving down to the bottom. 05:46 And you will notice upon closer examination, a beaded appearance. 05:52 Whereas when you take a look at the right, if your patient is suffering from gall stones, The most common gallstone will be your cholesterol stones right? Cholesterol stones and your cholesterol stones will be different, that FFFF means to say, fat female, forty, fertile. Those are cholesterol stones. 06:14 There is every possibility that you might accumulate bilirubin if at all your going to develop gall stones. 06:21 Then it will be a bilirubin type and it will be pigmented. 06:25 Imaging studies from ERCP- Endoscopic Retrograde Cholangio-Pancreatography Beaded appearance.
About the Lecture
The lecture Primary Sclerosing Cholangitis by Carlo Raj, MD is from the course Liver Diseases: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following is the histopathological characteristic of primary sclerosing cholangitis?
- Onion skin appearance
- Absence of bile ducts
- Fibrotic bands around the lobules of hepatocytes
- Non-caseating granulomas
- Lymphocytic infiltration limited to the portal triad only
Which of the following cancers are associated with primary sclerosing cholangitis?
- Colon cancer and cholangiocarcinoma
- Pancreatic carcinoma and cholangiocarcinoma
- Pancreatic adenocarcinoma and hepatocellular carcinoma
What is the radiological finding seen in primary sclerosing cholangitis?
- Beaded appearance
- Rat tail appearance
- Bird's beak appearance
- Double bubble sign
- Snowstorm sign
Author of lecture Primary Sclerosing Cholangitis

Carlo Raj, MD
Customer reviews
4,2 of 5 stars
| 5 Stars |
|
4 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
1 |
I was super confused about PBC and PSC but Dr. Raj made it clear! love his style of teaching
amazing lecture , i want tobe like doctor raj he is my hero
Great delivery of PBC. one of the best pathophysio professor for step 1 review
i dont know why but i dont like this lecturer in his slides here is lot of ontroversies slides says one thing and lecturer says another thing
1 customer review without text
1 user review without text
