Playlist
Show Playlist
Hide Playlist
Fulminant Liver Failure

-
Slides GD liver disease.pdf
-
Download Lecture Overview
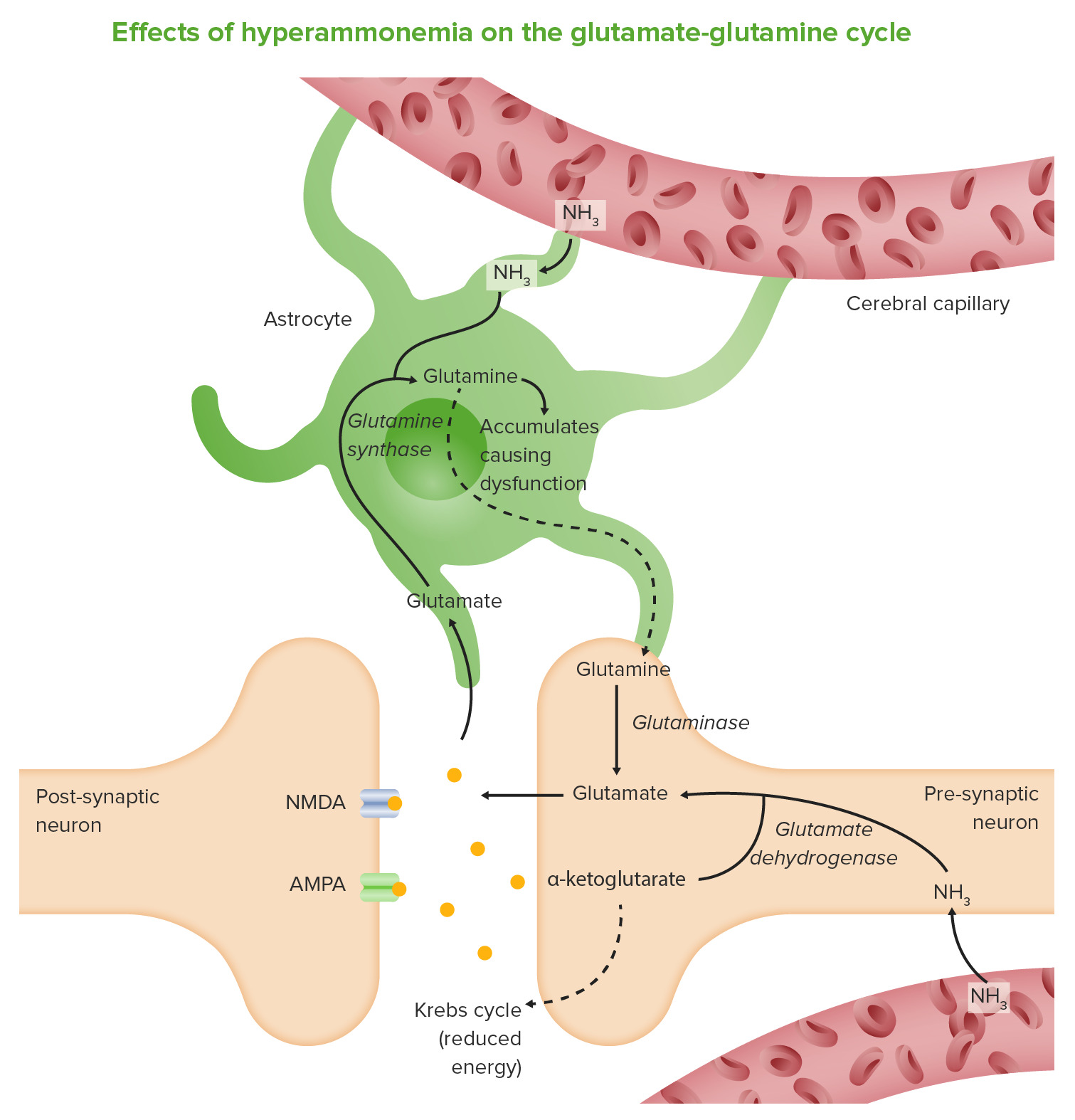
00:01 Our topic, fulminant liver failure. 00:04 This means that now, Liver failure has occurred in its overt nature. 00:10 All the different reasons is to why you might be going through liver failure well everything that causes liver failure extensively, Will go to liver failure and you call this a cirrhotic liver. Point of no return. 00:21 Hepatocellular dysfunction. 00:23 with encalopathy. 00:24 of jaundice without history of prior liver disease. 00:28 is Fulminant liver failure. 00:30 How important is this? Asterixis. 00:34 Really important. 00:36 Because this to you should indicate in a stem of a question, that your patient is going into or is in Fulminant liver failure. 00:48 Encaphalopathy, what does that mean to you? It means you have increased amounts of ammonia. 00:53 In the brain, resulting in encephalopathy. 00:55 In addition, there might be cerebral edema And with that cerebral edema in different types of herniation, might actually cause brain death. 01:05 presentation, complicated by sepsis. 01:09 hypotension, renal failure hypoglycemia coagulation or coagulopathy and hemmorage so a number of complications that you want to keep in mind the one that is really dangerous here will be sepsis, but the one that is dangerous here will be sepsis, but anyone of these, we'll talk about more of the sequelae as you progress through liver failure. 01:28 up to this point. we've talked about number of differentials that causes liver damage. 01:33 you take all these differentials and understand that if liver failure kicks in. 01:38 we will go in to sequelae and complications. 01:42 Etiology infections that we've talked about, viral. 01:45 Herpes in pregnancy, I've mentioned to you. 01:49 drugs, I talked about acetominaphens in great detail. 01:53 And, mushroom poisoning. 01:56 NAC by the way stand for n Acetylcysteine other causes, now this one, or this these set of differentials will be interesting let's just make sure we're clear. 02:10 vascular, resulting in Shock liver. What if you have something like Budd-Chiari? What's Budd-Chiari? it is specifically hepatic vein thrombosis. 02:23 Nothing else can be called Budd-Chiari unless you find thrombosis in the hepatic vein. 02:31 Be careful, students always get this confused And they forget, oh, of the thrombosis of the inferior vena cava. 02:38 that must be Budd-Chiari, no. 02:40 That is inferior vena cava thrombosis. That is not Budd-Chirai. 02:44 Is that clear? Metabolic causes of liver failure. 02:51 Wilson's disease? Let me ask you one question, Actually, I lied. 02:57 Two questions. 02:58 What is your total copper in Wilson's disease? Decreased. Good. 03:03 What is your free copper in Wilson's disease? Levels? Free increased. 03:08 Hence, you find it in the urine. 03:11 Acute Fatty liver of pregnancy. 03:14 A possible cause of fulminant liver failure. 03:20 Other differentials that we've talked about, Auto immune hepatitis. 03:24 Or at least know this. 03:25 Let me give you an acronym, L- Liver. 03:29 K- Kidney. 03:32 M- Microsome. 03:34 Know that as a possible marker for autoimmune hepatitis. 03:39 L-Liver K-Kidney, M-Microsome. 03:44 Massive Malignant infiltration. 03:47 This is not something to be taken at lightly, What is the most common causes of cancer in many organs? Metastasis. 03:56 Metastasis So if you are thinking about co-rectal cancer, the number sight for its metastasis would be the liver. 04:05 the malignant infiltration causing Fulminant liver failure. 04:10 Are we clear? Some of the important differentials that may result in liver failure. 04:19 On this table, we will compare and contrast acetaminophen toxicity and non acetaminophen toxicity Let's begin. 04:29 Acetominophen toxicity warrants its own discussion. 04:33 Because it is one of the most common causes of hepatitis. 04:36 And could be the leading cause of liver transplants in some patients. 04:41 Especially the young. 04:43 Acetominophen toxicity you find your Arterial pH to be perhaps decreased at 7.3 all through of the following: A PT increased. 04:55 And greater than 100 seconds. 04:57 What is normal? 11-15. 05:01 Creatinine A kidney could be involved. 05:05 We'll talk about this in a little bit. 05:08 What is normal creatinine? 0.6 to 1.2 3.4 or greater that is significant. 05:18 Right? And then encephalopathy Anytime that you have encephalopathy at this point, yes there is grade 3 or 4. 05:26 Always understand though if encephalopathy kicks in and yes there will be edema and asterixis This is not good. 05:33 Non-acetominophen A PT greater than 100 or any of the three. 05:39 Drug or non-viral hepatitis, Jaundice, greater than 7 days. 05:45 Age, less than ten years. 05:48 or greater than 40 years old. 05:49 A PT greater than 50 seconds. 05:52 or bilirubin being elevated. 05:55 So, two major list of criteria in which you would know as to whether or not your patient is suffering from quickly, Acetominophen toxicity take a look at that arterial pH lest than 7.3. 06:07 Or Non-acetominophen, all the differentials and perhaps three of the following. 06:14 From henceforth, you do not take acetominophen poisoning lightly. 06:19 It warrants its own discussion. 06:20 And has its own criteria Because you cannot afford to miss Fulminant liver failure if you have a patient coming through that door with acetominophen toxicity. 06:32 You have to establish diagnosis ASAP. 06:38 Now, all of these comes under to what we call King's college criteria. 06:41 are indicators of poor prognosis and need for liver transplantation.
About the Lecture
The lecture Fulminant Liver Failure by Carlo Raj, MD is from the course Liver Diseases: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following is NOT a part of the definition of fulminant hepatitis?
- The patient must have portal hypertension.
- The patient has a history of jaundice.
- Hepatic encephalopathy is present.
- The patient must present within 8 weeks.
- The patient has no prior history of liver disease.
Which of the following is NOT a sequela of fulminant hepatic encephalopathy?
- Fatty liver disease
- Brain herniation
- Renal dysfunction
- Coagulopathy
- Hypoglycemia
Author of lecture Fulminant Liver Failure

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
