Playlist
Show Playlist
Hide Playlist
Trauma: Primary Survey, Airway & Breathing



-
Emergency Medicine Trauma.pdf
-
Download Lecture Overview
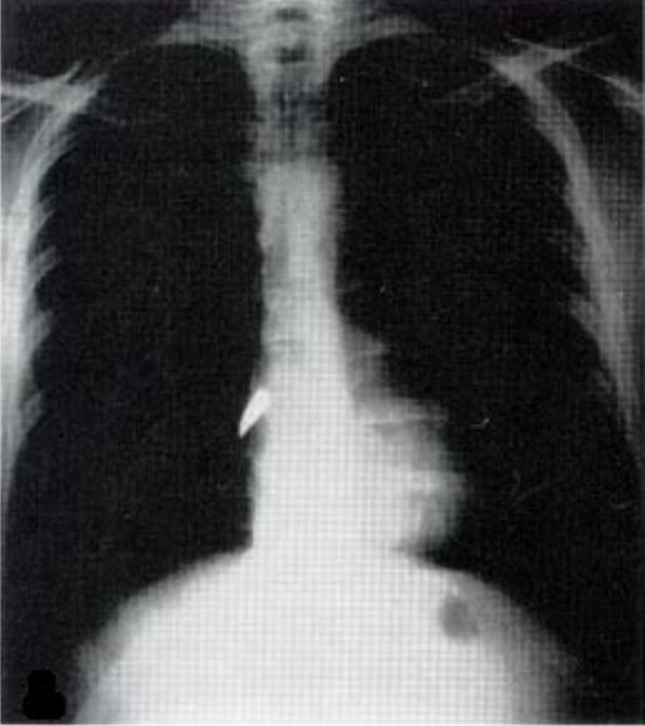
00:01 Hello. Now we are gonna talk about the overall approach to the traumatically injured patient. 00:06 Management of trauma always begins with the primary survey. 00:13 The primary survey is a standardized way of performing your initial assessment of all trauma patients and it should be done exactly the same way every single time in every single case so you don’t miss anything. 00:25 There are two major goals of the primary survey, one, is to identify life threats quickly and two is to provide stabilization when life threats are identified. 00:37 It’s very important to remember that the primary survey isn’t just about diagnosis, it involves simultaneous assessment and treatment of the patient to ensure that they remain stable and that life threats are quickly addressed. 00:50 The primary survey follows the same order every time. 00:54 It begins with airway followed by breathing, circulation, disability and lastly exposure of the patient and assessment of the environment. 01:05 So when we talk about assessing the airway, the first thing to do is simply speak to the patient, gasp them their name, get them to tell you what happened to them. 01:15 Any patient who’s able to talk by definition has a patent airway and that’s clearly a good sign. 01:21 However, remember just because you have a patent airway right now doesn’t mean you’re gonna have a patent airway 15 or 30 minutes from now, so you wanna not only identify current airway obstruction but also risks for potential future airway obstruction. 01:37 What if the patient is not actually talking to you? Well, the question you should ask yourself is why? If the patient is unconscious or unresponsive, then that suggest a head injury and if they have a significantly depressed GCS you probably wanna go ahead and provide definitive airway management in the form of intubation. 01:56 If the patient is conscious but they’re unable to phonate, they’re trying to speak but they’re -- this is a sign of significant airway injury and you wanna make sure that you address that quickly. 02:10 This is a situation where you’re gonna want to emergently intubate the patient or otherwise manage the airway if intubation is impossible. 02:19 So what are the kinds of things we’re looking for in terms of airway life threats? Well, for patients who have a currently patent airway but you wanna know whether they are gonna lose their airway in the future, things you wanna look for are swelling -- so any kind of hematoma in the face and neck, any kind of edema in the face or neck -- these can compress the airway. 02:41 You wanna look for bleeding in particular nasopharyngeal bleeding that’s going from the pharynx back into the oral cavity can cause aspirations. 02:50 We wanna be aware of that and address it. 02:52 And then lastly we want to palpate for crepitus and we do that by feeling for that crispy, crunchy feeling in the neck and upper chest. 03:00 This suggests some kind of injury to the airway structures either the larynx or the trachea which again would mandate definitive airway management. 03:09 While we’re thinking about the airway, we always want to think about the cervical spine. 03:14 So the cervical spine should be immobilized in trauma patients in case they do have an injury and anytime a patient has a high C-spine injury, they can actually lose their respiratory drive. 03:26 There’s a rhyme, C3, 4, 5 keeps the diaphragm alive - so patients who have injuries in those regions of the spinal cord might have impaired respiration not because of an airway problem but because of difficulty breathing from diaphragmatic paralysis. 03:42 Lastly, we just want to think about burns. 03:45 We have a whole separate lecture about burns and we’ll talk about the burned airway there, but for patients who do have any kind of burn as part of their trauma, you wanna just remember that thermal injury can cause airway edema and inhalational injury can cause damage to the lungs which in turn can make the patient hypoxic. 04:02 So these are all things that you want to think about for the airway of an injured patient. 04:07 Whenever you do identify airway compromise either currently or you think it’s gonna eminently develop, you wanna go ahead and intubate your patient, however, in trauma, there’s often distortion of the normal anatomy if the patients has swelling or bleeding or facial fractures, those kinds of things, the airway might be very technically challenging and to further add to our technical challenges we have to maintain spinal immobilization. 04:35 We can’t just crank the patient’s neck at any direction because we don’t know whether or not they have an underlying injury, so you need to be really proficient with airway management if you are gonna tackle a trauma airway and if this isn’t something you have a lot of experience with you probably wanna get back up from an anaesthesiologist although for emergency physicians of course we would expect this is something you’d be able to handle. 04:58 Always bear in mind that if you’re unable to intubate successfully in a noninvasive way, you need to think about the possibility of a surgical airway, so a surgical cricothyrotomy would be the procedure we would use for patients who have severe facial or neck injuries that preclude intubation and again if you’re gonna be managing trauma airways, this is a procedure that you need to master. 05:22 Now, we’re gonna move on to breathing and I’ll tell you in my 15 years of practice experience, I can tell you that traumatic injuries to the airway are actually relatively rare. 05:35 I’ve only seen a handful in all my years of practice, whereas, pulmonary injuries, chest injuries that lead to respiratory compromise - these are very common and these are something that you see regularly in the emergency department. 05:47 So airways are incredibly important and airway injuries are really life threatening but breathing is where you’re gonna find more pathology and more often need to intervene. 05:57 When you are assessing a patient’s breathing in trauma, one of the first things you wanna do is listen to their breath sounds bilaterally, and what you're listening for are the presence of equal bilateral breath sounds on both sides of the chest. 06:11 You also wanna look and just get an overall feel for their respiratory effort. 06:16 Of course, you’re gonna note the respiratory rate and you’re probably gonna pay attention to specifically what they’re doing when they’re breathing but at the beginning, if you just got a visceral sense of whether they’re kinda chilling, breathing comfortably, or if they’re working really hard to breathe, they’re using additional muscles and they’re having to pull air in, that should give you a sense of the severity of their respiratory compromise. 06:42 You of course want to count the respiratory rate, again, this is a vital sign that is often documented incorrectly and one that you really wanna double check your self and you should always be concerned about a patient with significant tachypnea because that’s somebody who could tire out and really get themselves into trouble shortly. 07:00 And then lastly, your respiratory vital sign is your oxygen saturation. 07:05 The whole purpose of the lungs is to get oxygen into the blood so you need to know if they are fulfilling that purpose effectively or not. 07:14 While we’re assessing breathing, we wanna be looking for evidence of pulmonary life threats and there are four major ones we wanna think about. 07:22 Tension pneumothorax is by far the most common and most serious in the trauma setting but you can also see open pneumothoracies, flail chest which is always associated with underlying pulmonary contusion, and then massive hemothorax. 07:37 Whenever you suspect that a patient has a compromised of their breathing, we always want to initiate supplemental oxygen. 07:46 You should give then whatever flow they need to keep their oxygen saturation normal which is typically gonna be above 95% for somebody with healthy lungs. 07:55 You also want to initiate emergency treatment for any patient in whom you identify a life threatening pulmonary injury. 08:03 Now we have a whole other lecture on chest trauma and I'm not gonna get into each of these too much right now, but there are immediate interventions for each one of these injuries that you can perform during the primary survey to stabilize your patient. 08:18 Once your patient is stable and you're satisfied you don’t have an immediate life threat in the pulmonary domain, we wanna get a chest x-ray to evaluate their lungs and get a sense of what’s going on with them from a pulmonary injury standpoint but we don’t wanna be getting chest x-rays until we’re satisfied that the patient is stable.
About the Lecture
The lecture Trauma: Primary Survey, Airway & Breathing by Julianna Jung, MD, FACEP is from the course Trauma (Emergency Medicine). It contains the following chapters:
- Primary Survey — ABCDE
- Airway
- Breathing
Included Quiz Questions
For a trauma patient presenting to the ED, which of the following is an indication to intubate?
- Inability to phonate
- Talking clearly but without making sense
- Respiratory rate of 16 breaths per minute
- GCS score of 12
- Oxygen saturation of 92%
What is the cause of respiratory impairment in cervical spine injuries at levels C3 to C5?
- Diaphragmatic paralysis
- Injury to the mainstem bronchi
- Tracheal collapse
- Laryngeal paralysis
- Esophageal expansion
What is the recommended airway management for trauma patients with severe facial and neck injuries?
- Surgical cricothyrotomy
- Nasotracheal intubation
- Needle cricothyrotomy
- Laryngeal mask airway
- Orotracheal intubation
What is the most common and most serious pulmonary life threat observed in trauma patients?
- Tension pneumothorax
- Open pneumothorax
- Flail chest
- Massive hemothorax
- Atelectasis
Which of the following statements regarding the primary survey is NOT true?
- It involves arriving at the correct diagnosis at the time of the assessment.
- It is the standardized initial assessment of all trauma patients.
- It includes assessment of the airway, breathing, and circulation.
- One of its goals is to identify life threats.
- One of its goals is to provide immediate stabilization.
Which of the following is NOT a part of the breathing assessment?
- Percussion of the abdomen
- Look for gestalt respiratory effort.
- Listen for equal bilateral breath sounds.
- Count for respiratory rate.
- Monitor for oxygen saturation.
Author of lecture Trauma: Primary Survey, Airway & Breathing

Julianna Jung, MD, FACEP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I like it because focusses in a practical way, so concise and easy to learn. Good to get overview of the theme.
